







{kind=link}
{kind=link}
{kind=link}
INTRODUCTION
Early and accurate parasitological diagnosis is the cornerstone of malaria treatment and control strategy. Light microscopy performed on peripheral blood smears remains the reference standard for malaria diagnosis. 1 Malaria rapid diagnostic tests are often in use in routine care in malaria-endemic regions. Microscopy offers the advantages of differentiating malaria parasite species and stage along with the quantification of peripheral blood parasitemia. 2 However, light microscopy is not easy to adapt to settings where laboratory infrastructure and resources for quality assurance are limited, as is often the case in malaria-endemic areas. Standardization is further hindered by variability in the quality and procedures for slide preparation and staining, as well as differences in the number of thick film fields examined or white blood cells (WBCs) counted to detect or quantify parasitemia, leading to considerable variation in the performance of field-based malaria microscopy. 3–5
Microscopic examination of stained blood smears has become the standard of malaria diagnosis since the introduction of Giemsa’s solution in 1904. 6,7 Giemsa stains’ stability and its persistent staining quality made it preferable over other stains, that is, Leishman, Field, Romanowsky, or Wright stain. 8,9 There are two methods of staining with Giemsa stain: rapid and slow methods. The rapid method (10% Giemsa solution, stain for 10–15 minutes) is generally used in outpatient clinics and busy laboratories where a quick result is required to determine a patient’s malaria status. The slow method (3–5% Giemsa solution, stain for 45–60 minutes) is often used for staining a large number of slides and is ideal for staining blood smears from surveys or clinical research studies. Evidence suggests that large numbers of parasites can be lost during rapid staining procedures, which might result in errors in parasite detection and density estimation. 10,11
Accurate parasite quantification is essential for the management of malaria patients by assessing disease severity associated with high parasitemia, and for testing antimalarial drug resistance and monitoring drug-efficacy. 12 Parasite density can be estimated by counting parasites against WBCs (WBC method) or per oil immersion field (high-power field, HPF method) on a thick smear or against red blood cells (RBC method) on a thin smear. Variability in blood film reading procedures accounts for considerable variation in parasite counts. Such variability might substantially affect research outcomes and end point determination in antimalarial drug efficacy trials, as well as in asymptomatic and submicroscopic infections. 13 For instance, the time from antimalarial treatment administration until no asexual malaria parasites are detectable in a peripheral blood smear, that is, the parasite clearance time, is generally considered to be an essential measure of antimalarial treatment efficacy. 14 The amount of blood examined on a blood smear is also crucial because the likelihood of detecting a malaria infection is a function of the blood volume considered. 11,15 Thus, the method to declare a peripheral blood smear negative is important for study outcomes. Although guidelines and manuals for malaria microscopy methods have been developed under the umbrella of the WHO, there is an often-expressed need for practical recommendations for standardized reporting of malaria microscopy procedures. 1,16,17
The purpose of this review was to explore critically how malaria microscopy methods and results were documented in malarial clinical trials published in 2013–2017. We also aimed to outline the methodological variations observed in the microscopy procedures.
MATERIALS AND METHODS
Search strategy and selection criteria.
The current review was conducted using the “WorldWide Antimalarial Resistance Network (WWARN) Clinical Trials Publication Library,” an open-access, up-to-date database of malaria treatment efficacy trials, as a resource. 18 In brief, the WWARN publication library was constructed using a series of searches in PubMed, Excerpta Medica Database, and Web of Science Core Collection databases to identify prospective clinical trials assessing antimalarial drug efficacy. 19 In this current review, all studies published between 2013 and 2017 (5 years) and listed in the “WWARN Clinical Trials Publication Library” were deemed eligible for inclusion. The authors assumed that all prospective clinical studies published in these 5 years would be representative of the current microscopy methods practiced in field malaria drug trials. Those selected articles were examined in depth to explore how the microscopy procedures were performed and documented.
Data extraction.
For the selected articles, full texts were obtained, and two reviewers (D. D., P. D.) extracted relevant variables of interest. From each of the included studies in this review, the following variables related to the malaria microscopy method were extracted (when available): slide staining method, Giemsa stain strength, duration, parasite density estimation, gametocyte count method, the method to declare slide negative, and quality control (QC) procedures. The details on extracted variables are presented as the data dictionary in Supplemental File 1. The first reviewer (D. D.) independently extracted the data using Research Electronic Data Capture (REDCap, Vanderbilt University, Nashville, TN), an online data capture tool hosted at the University of Oxford. 20,21 The second reviewer (P. D.) double-checked and verified the data extracted by the first reviewer on all publications included in the review. Any discrepancy in the extracted information was flagged within the REDCap system by the second reviewer. The differences were resolved through consensus between the two reviewers.
Data definition.
While extracting parameters related to the microscopy method, the information not available in the full-text article or in the Supplemental File was recorded as “not stated.” The reported methodological variations were also stratified by parasite species and study location. Parasite species were grouped into Plasmodium falciparum only, Plasmodium vivax only, both species (P. falciparum or P. vivax or mixed), or other species (Plasmodium malariae, Plasmodium ovale, and Plasmodium knowlesi). Study locations were grouped into regions according to the United Nations designation of areas and regions. 22
Data analysis.
Variations in microscopy methods and results are presented as descriptive statistics in this review. The primary unit of the analysis reported in the Results section is “publication.” Data were analyzed using R software, version 3.6.3 (The R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
A total of 206 published malaria studies between 2013 and 2017 from the “WWARN Clinical Trials Publication Library” were selected and assessed in full-text in this review (Figure 1). Of the 206 published studies, 51% (104/206) were conducted in Africa, 38% (78/206) in Asia, 8% (17/206) in the Americas, and 3% (7/206) were multiregional. Besides, 66% (135/206) studies recruited patients with P. falciparum only, 23% (48/206) with P. vivax only, 9% (18/206) with both species, and 2% (5/206) with other species (Supplemental File 2).

Study flow diagram.
Citation: The American Journal of Tropical Medicine and Hygiene 104, 3; 10.4269/ajtmh.20-1219
Method for parasite density estimation.
The approaches for parasite density estimation, as reported in the 206 malaria articles derived from the WWARN Clinical Trials Publication Library, are summarized in Table 1 and Figure 2.
Estimation of parasitemia per µL using the WBC method (N = 125)
| Variable | N | % |
|---|---|---|
| Actual WBC count/µL* | 11 | 8.8 |
| Assumed WBC count/µL | ||
| 6,000 WBCs | 16 | 12.8 |
| 7,000 WBCs | 1 | 0.8 |
| 7,500 WBCs | 2 | 1.6 |
| 8,000 WBCs | 85 | 68 |
| 10,000 WBCs | 1 | 0.8 |
| Not stated | 9 | 7.2 |
N = number of articles; WBC = white blood cells.
Actual WBC count was measured using a hematology analyzer.
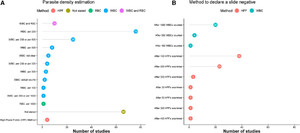
Methodologies used for parasite density estimation and for declaration of a slide negative (N = 206 articles). HPFs = high-power fields; RBC = red blood cells; WBC = white blood cells. “WBC: per X” means X WBCs were counted.
Citation: The American Journal of Tropical Medicine and Hygiene 104, 3; 10.4269/ajtmh.20-1219
Asexual peripheral parasitemia.
Of the 206 studies, 61% (125/206) estimated parasite density by the WBC method, 2% (4/206) by the HPF method, a single study used the RBC method, and 5% (10/206) used both WBC and RBC methods (Figure 2A). About one-third of the articles (32%, 66/206) did not report the method for parasitemia estimation. Among studies in which peripheral parasitemia was measured using the WBC method, 37% counted parasite densities per 200 WBC, 4% per 500 WBC, and 12% per 200 or 500 WBC. To calculate parasite density per µL, the majority of studies (84%, [105/125]) used an assumed WBC value per µL, whereas only 9% (11/125) used an actual count of WBC measured by using the hematology analyzer. In studies calculating parasitemia using assumed WBC values, the range was 6,000–10,000 WBCs/µL, with 68% (85/125) assuming 8,000 WBCs/µL and 16/125 (13%) using 6,000 WBCs/µL (Table 1). The reported methods for parasite density estimation stratified by study region and parasite species are shown in Table 2.
Reported methodology used for estimating parasite density (N = 206)
| Methodology used for estimating parasite density | ||||||
|---|---|---|---|---|---|---|
| N | WBC | RBC | WBC and RBC | High-power fields | Not stated | |
| Region | ||||||
| Africa | 104 | 71 (68.3%) | 0 (0.0%) | 1 (1.0%) | 3 (2.9%) | 29 (27.9%) |
| Asia | 78 | 39 (50.0%) | 1 (1.3%) | 9 (11.5%) | 0 (0.0%) | 29 (37.2%) |
| The Americas | 17 | 12 (70.6%) | 0 (0.0%) | 0 (0.0%) | 1 (5.9%) | 4 (23.5%) |
| Multiregional | 7 | 3 (42.9%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 4 (57.1%) |
| Parasite species | ||||||
| P. falciparum | 135 | 93 (68.9%) | 0 (0.0%) | 2 (1.5%) | 3 (2.2%) | 37 (27.4%) |
| P. vivax | 48 | 24 (50.0%) | 0 (0.0%) | 3 (6.2%) | 1 (2.1%) | 20 (41.7%) |
| P. falciparum and P. vivax | 18 | 6 (33.3%) | 1 (5.6%) | 5 (27.8%) | 0 (0.0%) | 6 (33.3%) |
| Other | 5 | 2 (40.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 3 (60.0%) |
| Overall | 206 | 125 (60.7%) | 1 (0.5%) | 10 (4.9%) | 4 (1.9%) | 66 (32.0%) |
N = number of articles; P. falciparum = Plasmodium falciparum; P. vivax = Plasmodium vivax; row percentages are presented within the parenthesis; RBC = red blood cells; WBC = white blood cells.
Method to consider slide negative.
More than half of the studies (55%, 113/206) did not mention how a patient was considered aparasitemic by microscopy examination (Figure 2B). One-third (33%, 68/206) of studies used the HPF method in which microscopic fields ranging from 30 to 500 were examined before declaring a slide negative. Examining 100 HPFs (56%, 38/68) was the most common method reported, followed by 200 HPFs (34%, 23/68). And, 12% of studies (25/206) followed the WBC method, whereby 1,000 WBCs were examined before considering a slide negative most often (80%, 20/25). The methods for declaring a slide negative stratified by study region and parasite species are shown in Table 3.
Reported methods to declare a slide negative (N = 206)
| Methodology used to declare a slide negative | ||||
|---|---|---|---|---|
| N | High-power field | White blood cell | Not stated | |
| Region | ||||
| Africa | 104 | 46 (44.2%) | 7 (6.7%) | 51 (49.0%) |
| Asia | 78 | 15 (19.2%) | 14 (17.9%) | 49 (62.8%) |
| The Americas | 17 | 6 (35.3%) | 3 (17.6%) | 8 (47.1%) |
| Multiregional | 7 | 1 (14.3%) | 1 (14.3%) | 5 (71.4%) |
| Parasite species | ||||
| P. falciparum | 135 | 55 (40.7%) | 16 (11.9%) | 64 (47.4%) |
| P. vivax | 48 | 11 (22.9%) | 8 (16.7%) | 29 (60.4%) |
| P. falciparum and P. vivax | 18 | 2 (11.1%) | 1 (5.6%) | 15 (83.3%) |
| Other | 5 | 0 (0.0%) | 0 (0.0%) | 5 (100.0%) |
| Overall | 206 | 68 (33.0%) | 25 (12.1%) | 113 (54.9%) |
N = number of articles; P. falciparum = Plasmodium falciparum; P. vivax = Plasmodium vivax; row percentages are presented within the parenthesis; WBC = white blood cells.
Staining of blood smear.
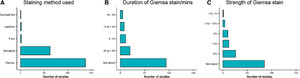
Of the included studies, 67% (138/206) used Giemsa-stained blood films for microscopic examination, whereas in one-third (63/206), information on the staining procedure was not available (Figure 3A). The strength of Giemsa stain ranging from 2 to 10% and duration of staining ranging from 5 to 60 minutes were reported (Figure 3B and C). Studies using 10% Giemsa solution (rapid) stained slides for 10–30 minutes, except for a single study that used a 5-minute staining duration. Studies using 3% Giemsa solution (slow) stained slides for 30–60 minutes.
Blood film staining procedures (N = 206 articles).
Citation: The American Journal of Tropical Medicine and Hygiene 104, 3; 10.4269/ajtmh.20-1219
Quality control procedures.
Of the 206 articles reviewed, two-thirds (135/206) reported some form of QC procedures, that is, the proportion of slides cross-checked and/or sent to a reference laboratory for external QC. However, in about one-third published articles (70/206), there was no mention of any cross-checking system in place to assess blood film preparation, stain quality, parasite detection, and quantification—the critical components of a quality assurance system for malaria microscopy. Only 14 studies in this review explicitly stated how discrepancies between two microscopists were resolved. The reported QC procedures stratified by study region and parasite species are shown in Table 4.
Quality control procedures reported (N = 206)
| Reporting of QC procedures | ||||
|---|---|---|---|---|
| Region | N | QA/QC carried out | QA/QC not carried out | Not stated |
| Africa | 104 | 73 (70.2%) | 1 (1.0%) | 30 (28.8%) |
| Asia | 78 | 44 (56.4%) | 0 (0.0%) | 34 (43.6%) |
| The Americas | 17 | 12 (70.6%) | 0 (0.0%) | 5 (29.4%) |
| Multiregional | 7 | 6 (85.7%) | 0 (0.0%) | 1 (14.3%) |
| Parasite species | ||||
| P. falciparum | 135 | 93 (68.9%) | 1 (0.7%) | 41 (30.4%) |
| P. vivax | 48 | 29 (60.4%) | 0 (0.0%) | 19 (39.6%) |
| P. falciparum and P. vivax | 18 | 11 (61.1%) | 0 (0.0%) | 7 (38.9%) |
| Other | 5 | 2 (40.0%) | 0 (0.0%) | 3 (60.0%) |
| Overall | 206 | 135 (65.5%) | 1 (0.5%) | 70 (34.0%) |
N = number of articles; P. falciparum = Plasmodium falciparum; P. vivax = Plasmodium vivax; row percentages are presented within the parenthesis; QC = quality control.
A checklist for reporting microscopy methods and results in malaria study publications.
|
DISCUSSION
We have documented differences in microscopic procedures adopted in malaria clinical trials in terms of slide staining, parasite density estimation, the method to declare a slide negative, and QC procedures. The observed differences could not be statistically explained by differences in parasite species or study location, indicating a generalized lack of standardization in the methods used and their reporting. Further detailed exploration was limited by the large proportion of studies, about one-third to half, with missing information (referred to as “not stated”) on the parameters related to the microscopy. However, a tendency toward more comprehensive reporting on methods was observed in studies conducted in Africa compared with those in Asia (Tables 2 and 3).
Poor staining techniques have the potential to generate artifacts commonly mistaken for malaria parasites: stain precipitation, presence of dirt, and cellular debris, resulting in a false-positive diagnosis. 9 Such misdiagnosis may cause unnecessary use of antimalarial drugs and their potential adverse effects in routine clinical practice, as well as has implications for determining the effectiveness of antimalarial drugs. 17 Thus, high-quality smear preparation and staining are required to ensure diagnostic accuracy and correct assessment of parasite density. For more transparency on staining procedures, as minimum information, the type of stain, the strength, and duration of staining should be systematically reported. Moreover, the standardized, automated blood slide preparation and staining merit further investigation to address the inherent inconsistencies in procedures. 23
Microscopic examination of the thick blood film, first introduced by Ross and Thomson 24 , is still the method of choice for examining blood for malaria parasites and estimating the parasite density in field studies. The method of choice for parasite density estimation is dependent on the level of parasitemia. Therefore, the methods used for parasite quantification can vary not only between the studies but also within a study. Different approaches were practiced for counting parasites on thick blood films, as evidenced in this review (Table 2). Parasite count is not only important for the assessment of the severity of malaria but also crucial for monitoring the therapeutic efficacy of drugs, emergence, and spread of drug resistance. 25 Efficacy outcomes depend on parasite clearance estimates and on the accurate determination of parasitemia status during follow-up.
Parasite density estimation varies with the total WBC count per microliter used in the calculations. 26,27 In a given population, WBC counts generally vary and are age-dependent. Olliaro et al. 28 highlighted an inverse relationship between age and actual WBC counts in African children younger than 5 years with uncomplicated P. falciparum malaria. The study also showed an underestimation of parasitemia in infants compared with the older age-groups, whereas assumed white cell counts of 8,000/µL were used to estimate parasite density. Values of severalfold fluctuations in total WBC counts in the African population have also been reported. 29,30 Many laboratories in malaria-endemic remote settings may not have the technical capacity to measure actual WBC counts. Quite paradoxically, our review had also found that the actual WBC measurements are not always used for estimation of parasite density even when they were measured. Of 125 studies that used the thick-film method in the current review, 84% (105/125) used assumed WBC counts to estimate parasite density, although at least 10% (10/105) of those studies measured actual WBC counts. Getting the patient's actual WBC count and enumerating the number of parasites per WBC can provide an accurate method of estimating parasite density. 31 The HPF method (the parasite density calculated from the average number of parasites present per HPF, and the estimated volume of blood present in one HPF) has proved to be more accurate than the WBC method for determining malaria parasite count, given the correct volume of blood is used in the preparation of thick blood smear. 29 However, despite the improved accuracy, the current review showed that the HPF method for density estimation is seldom practiced in field microscopy.
The method to declare a slide negative is critical in parasite clearance studies and field therapeutic efficacy studies in which blood films are examined daily. For instance, if blood films are taken daily and a microscopist fails to detect a single parasite in the thick blood film, then the parasite clearance time could be reduced by 24 hours. Of the reviewed studies, only 11% (23/206) counted 200 HPFs as per the WHO Research Malaria Microscopy Standards before declaring a patient aparasitemic. 1 Even if the number of HPFs is standardized, there is a need for standard thick films and microscope because the volume of blood examined varies with the thickness of the films and the size of the HPF.
Our review has some limitations. Information on microscopy methodology was primarily extracted from the full-text articles. If a full-text referred to a Supplemental File, that was also searched for. However, study protocols were not accessible to extract the intended parameters. In some articles, microscopy procedures were not described in the text and instead referred to the WHO guidelines and manuals, which can partially explain the large number of “not stated” parameters. In addition, some studies, focusing solely on parasite clearance measures such as slope half-life or the proportion of patients remaining parasitemic on day 3, might have been excluded because of the inclusion criteria of a minimum 28 days of follow-up in the WWARN Clinical Trials Publication Library. However, it is unlikely that this selection criterion may have caused an information bias. The review was conducted over a period of 5 years, from 2013 through 2017. We believe that this period would be representative of current microscopy practices, and it is unlikely that those practices have substantially changed since.
The observed differences in microscopy methods need to be minimized by implementing standardized procedures. This would allow for methodological consistency and comparability of clinical trial outcomes across studies. Based on the findings of this review, we have proposed a minimum checklist for reporting microscopy procedures and results in malaria study publications (Box 1). This evidence-based checklist supplements existing guidelines and recommendations for microscopy methods. 1,17 We propose pursuing the following standard practices: a minimum of 200 HPFs should be examined on the thick film before declaring a slide negative. Parasites should be estimated against 500 WBCs in the thick film, given actual WBC counts by a hematology analyzer is used for counting parasitemia. If the laboratory facility to perform actual WBC counts is not available, parasites must be counted in 40 HPFs on the thick smear. Another provision for the adoption of a harmonized standard microscopy procedure would be making it a prerequisite by the sponsor or funder of a trial.
CONCLUSION
Our review documents heterogeneity in malaria microscopy procedures and the need for following standardized approaches in malaria clinical trials. The authors have captured a range of variations in current field malaria microscopy practice and highlighted how this observed variability might lead to considerable differences in malaria diagnosis and parasite density estimation. This study aimed to provide an overview of the principles and approaches used in malaria microscopy methods and suggest a checklist of items to be systematically reported in future studies. Researchers and policy-makers should discuss and agree on strategies toward harmonization of the microscopy procedures.
ACKNOWLEDGMENTS
We thank Junko Takata, Paul Sondo, Sharif Hossain, and Elke Wynberg for their invaluable assistance with the WWARN Clinical Trials Publication Library.
REFERENCES
- 1.↑
Research Malaria Microscopy Standards Working Group , 2015. Microscopy for the Detection, Identification and Quantification of Malaria Parasites on Stained Thick and Thin Films. Geneva, Switzerland: World Health Organization.
- 2.↑
White NJ , Krishna S , 1989. Treatment of malaria: some considerations and limitations of the current methods of assessment. Trans R Soc Trop Med Hyg 83: 767–777.
- 3.↑
O’Meara WP , Barcus M , Wongsrichanalai C , Muth S , Maguire JD , Jordan RG , Prescott WR , McKenzie FE , 2006. Reader technique as a source of variability in determining malaria parasite density by microscopy. Malar J 5: 118.
- 4.
Mahende C , Ngasala B , Lusingu J , Yong TS , Lushino P , Lemnge M , Mmbando B , Premji Z , 2016. Performance of rapid diagnostic test, blood-film microscopy and PCR for the diagnosis of malaria infection among febrile children from Korogwe District, Tanzania. Malar J 15: 391.
- 5.↑
Wilson ML , 2013. Laboratory diagnosis of malaria: conventional and rapid diagnostic methods. Arch Pathol Lab Med 137: 805–811.
- 6.↑
Giemsa G , 1904. Eine Vereinfachung und Vervollkommnung meiner Methylenblau‐Eosin‐Färbemethode zur Erzielung der Romanowsky‐Nocht’schen Chromatinfärbung. Centralblatt für Bakteriologie I Abteilung 32: 307–313.
- 7.↑
Nocht B , 1899. Zur Färbung der Malariaparasiten. Centralblatt für Bakteriologie I Abteilung 25: 764–769.
- 8.↑
Fleischer B , 2004. Editorial: 100 years ago: Giemsa’s solution for staining of plasmodia. Trop Med Int Health 9: 755–756.
- 10.↑
Bejon P , Andrews L , Hunt-Cooke A , Sanderson F , Gilbert SC , Hill AV , 2006. Thick blood film examination for Plasmodium falciparum malaria has reduced sensitivity and underestimates parasite density. Malar J 5: 104.
- 11.↑
Dowling MA , Shute GT , 1966. A comparative study of thick and thin blood films in the diagnosis of scanty malaria parasitaemia. Bull World Health Organ 34: 249–267.
- 13.↑
Mogeni P et al. 2017. Detecting malaria hotspots: a comparison of rapid diagnostic test, microscopy, and polymerase chain reaction. J Infect Dis 216: 1091–1098.
- 14.↑
Bruce-Chwatt LJ , 1981. Chemotherapy of Malaria, 2nd edition. Geneva, Switzerland: World Health Organization.
- 15.↑
Trape JF , 1985. Rapid evaluation of malaria parasite density and standardization of thick smear examination for epidemiological investigations. Trans R Soc Trop Med Hyg 79: 181–184.
- 16.↑
WHO , 2010. Basic Malaria Microscopy, 2nd edition. Geneva, Switzerland. World Health Organization.
- 17.↑
Dhorda M et al. 2020. Towards harmonization of microscopy methods for malaria clinical research studies. Malar J 19: 324.
- 18.↑
WWARN , 2020. WWARN Clinical Trials Publication Library. Available at: https://www.wwarn.org/tools-resources/literature-reviews/wwarn-clinical-trials-publication-library. Accessed June 15, 2020.
- 19.↑
Takata J , Sondo P , Humphreys GS , Burrow R , Maguire B , Hossain MS , Das D , Commons RJ , Price RN , Guerin PJ , 2020. The WorldWide antimalarial resistance network clinical trials publication library: a live, open-access database of Plasmodium treatment efficacy trials. Am J Trop Med Hyg 103: 359–368.
- 20.↑
Harris PA , Taylor R , Thielke R , Payne J , Gonzalez N , Conde JG , 2009. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 42: 377–381.
- 21.↑
Harris PA et al. 2019. The REDCap consortium: building an international community of software platform partners. J Biomed Inform 95: 103208.
- 22.↑
United Nations , 1970. Standard Country or Area Codes for Statistical Use (M49). Available at: https://unstats.un.org/unsd/methodology/m49/overview/. Accessed April 7, 2020.
- 23.↑
Murphy SC , Shott JP , Parikh S , Etter P , Prescott WR , Stewart VA , 2013. Malaria diagnostics in clinical trials. Am J Trop Med Hyg 89: 824–839.
- 24.↑
Ross R , Thomson D , 1910. Some enumerative studies on malaria fever. Ann Trop Med Parasitol 4: 267–313.
- 25.↑
Dondorp AM et al. 2009. Artemisinin resistance in Plasmodium falciparum malaria. N Engl J Med 361: 455–467.
- 26.↑
Prudhomme O’Meara W , McKenzie FE , Magill AJ , Forney JR , Lucas C , Gasser RA Jr. , Wongsrichanalai C , 2005. Sources of variability in determining malaria parasite density by microscopy. Am J Trop Med Hyg 73: 593–598.
- 27.↑
Prudhomme O’Meara W et al. 2006. Systematic comparison of two methods to measure parasite density from malaria blood smears. Parasitol Res 99: 500–504.
- 28.↑
Olliaro P , Djimde A , Karema C , Martensson A , Ndiaye JL , Sirima SB , Dorsey G , Zwang J , 2011. Standardised versus actual white cell counts in estimating thick film parasitaemia in African children under five. Trop Med Int Health 16: 551–554.
- 29.↑
Greenwood BM , Armstrong JR , 1991. Comparison of two simple methods for determining malaria parasite density. Trans R Soc Trop Med Hyg 85: 186–188.
- 30.↑
Shaper AG , Lewis P , 1971. Genetic neutropenia in people of African origin. Lancet 2: 1021–1023.