







{kind=link}
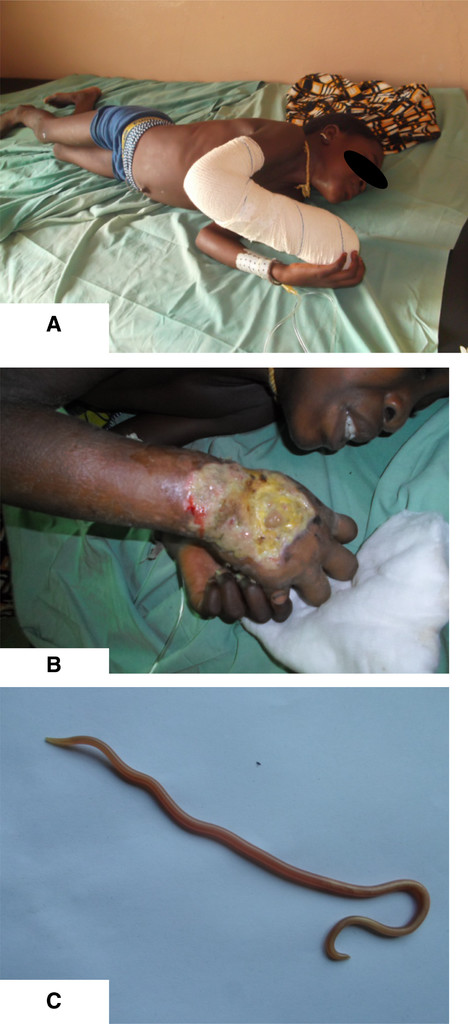
A 10-year-old girl was admitted in Benin (West Africa) with trismus, irritability, and fever. Physical examination revealed clinical findings compatible with tetanus, including a stiff neck, opisthotonus, risus sardonicus, and dysphagia (Figure 1A). On her right arm, she had an ulcer for 2 months. By IS2404 polymerase chain reaction,1 the ulcer was confirmed as Buruli ulcer, caused by Mycobacterium ulcerans, a neglected tropical disease (Figure 1B). The ulcer was treated with a black powder by a local traditional healer. We believe this procedure may have introduced the Clostridium tetani spores because 1 year ago, another Buruli ulcer patient presented with tetanus after a similar traditional treatment. The patient was treated in a quiet, dark room with equine antitoxin, metronidazol, and diazepam. She did not receive tetanus vaccinations in the past. The Buruli ulcer was initially treated with wound care and 8 weeks of rifampicin and streptomycin. Nine days after admission, an Ascaris lumbricoides crawled out of the patient's nose (Figure 1C). Adult worms tend to migrate in the presence of anesthetics or fever.2 We suspect her generalized tetanic spasms to have directed this worm toward her nose. Twenty-two days after admission, the generalized tetanic spasms abated. The ascariasis was treated with albendazole.

Poverty-related diseases attack simultaneously; tetanus, buruli ulcer and ascariasis.
Citation: The American Society of Tropical Medicine and Hygiene 94, 5; 10.4269/ajtmh.15-0823
The patient was discharged 10 months after admission because of a complicated treatment of the Buruli ulcer consisting of multiple debridements and skin grafting. There were no signs of osteomyelitis. This patient unfortunately has permanent functional limitations of her wrist as a consequence of Buruli ulcer. Permanent functional limitations are common in former Buruli ulcer patients, especially in patients with large ulcers.3
These three panels illustrate the fact that poverty-related diseases are coendemic and may lead to a synergistic threat to a persons' health.
- 1.↑
Stienstra Y, van der Werf TS, Guarner J, Raghunathan PL, Spotts Whitney EA, van der Graaf WT, Asamoa K, Tappero JW, Ashford DA, King CH, 2003. Analysis of an IS2404-based nested PCR for diagnosis of Buruli ulcer disease in regions of Ghana where the disease is endemic. J Clin Microbiol 41: 794–797.
- 2.↑
Gan RW, Gohil R, Belfield K, Davies P, Daniel M, 2014. Acute airway obstruction by Ascaris lumbricoides in a 14-month-old boy. Int J Pediatr Otorhinolaryngol 78: 1795–1798.
- 3.↑
Barogui Y, Johnson RC, van der Werf TS, Sopoh G, Dossou A, Dijkstra PU, Stienstra Y, 2009. Functional limitations after surgical or antibiotic treatment for Buruli ulcer in Benin. Am J Trop Med Hyg 81: 82–87.