










{kind=link}
{kind=link}
{kind=link}
{kind=link}
Introduction
The United Nations (UN) Interagency Group for Child Mortality Estimation (IGME) recently reported that, in 2011, 7.6 million children died worldwide before the age of 5 years, a reduction from 8.1 million deaths in 2008.1 Despite global progress in reducing child mortality rates, the average annual rate of reduction is low in many countries. Too few children are reached with effective interventions to treat common causes of death, such as pneumonia, malaria, and diarrhea.2 Training and deploying skilled community-based health workers (CBHWs) to provide quality childcare services can improve access to life-saving interventions, and the use of CBHWs is recommended by global policies.3,4 According to the World Health Organization (WHO), 39 of 74 countries with high maternal and child mortality had adopted a policy allowing CBHWs to treat pneumonia in the community by the end of 2012, 24 of which were located in sub-Saharan Africa.5 Countries that allow community management of pneumonia often also support the management of malaria and diarrhea in the community. A UNICEF survey conducted in the African region in 2010 found that, among 40 countries, 18 countries had established policies allowing CBHWs to treat pneumonia, diarrhea, and malaria.6 However, important questions have arisen about the quality, use, and impact of community child services.7,8
In 2008, the Government of Malawi (GoM) started a program to train an existing cadre of CBHWs, known as Health Surveillance Assistants (HSAs), to provide integrated community case management of childhood illness (iCCM). In this paper, we document progress in the scale up of iCCM between 2008 and 2011, describe some critical challenges that affect the effectiveness and sustainability of the program, and propose solutions. Because Malawi is one of the first sub-Saharan African countries to scale up iCCM for common child illnesses, we describe the experiences to contribute to the global understanding and learn about scaling up effective community child health services.
Context
Malawi is considered on track to achieve the Millennium Development Goal 4. Mortality among children less than 5 years of age decreased from 225 deaths per 1,000 live births in 1990 to 92 per 1,000 live births in 2010.1 Nevertheless, 53% of children under 5 years are stunted, and 4% are wasted.9 In 2006, only 27% of children with diarrhea received oral rehydration therapy, only 30% of children with suspected pneumonia received an antibiotic, and only 25% of children with fever received an appropriate antimalarial.10 Additionally, the percentage of infants born to human immunodeficiency virus (HIV)-positive mothers who are infected is estimated at 14%, although there is a steady increase in the proportion of pregnant women who are reached by prevention of mother-to-child transmission (PMTCT) interventions.11 Thus, a large proportion of children in Malawi are still at increased risk of mortality because of common childhood infections, such as malaria, pneumonia, and diarrhea.
In Malawi, access to health services is an important barrier to intervention coverage. An estimated 30–35% of the population lives more than 8 km from a health center, particularly in rural areas. In 2004, the GoM adopted a Plan of Action to strengthen health services that was centered around the delivery of an Essential Health Package (EHP).12 The EHP specifies community-based treatment of common childhood illnesses to be delivered free of charge.
Methods
This paper provides an overview of the implementation of CCM in Malawi, summarizing information from multiple data sources. The main sources of data were program records and Health Management Information System (HMIS) reports from the Integrated Management of Childhood Illness (IMCI) unit in the Ministry of Health (MOH), and they included statistics on the number of HSAs trained, the number of village health clinics (VHCs) established, the proportion of target areas reached, and the number of treatments provided by month. These data are compiled by the MOH from monthly reports provided by trained HSAs and reported through health facilities and the district health office on a monthly basis. The density of HSAs per 1,000 population (based on the Malawi 2009 census estimates of district population)13 and the ratio of functional VHCs per hard-to-reach area (as identified by the MOH) were calculated in Microsoft Excel.
We also include the results of additional assessments conducted for an external evaluation of maternal and child health programming in Malawi led by the Institute for International Programs at Johns Hopkins University (IIP-JHU) and the Malawi National Statistics Office (NSO), here referred to as the Independent Evaluation Team (IET). In 2009, the IET conducted an assessment of the quality of care provided by HSAs through direct observation and reexamination by a gold-standard clinician.14 The assessment also included measurement of caregiver satisfaction with CCM services through a client exit interview and qualitative investigation of health workers perceptions of the CCM program.14,15 The assessment was conducted in six districts that were strong in early implementation, and results are not representative of all districts during that period, which had variable implementation. The IET collected follow-up data on implementation strength in 2011 through a telephone survey of a random sample of CCM-trained HSAs in one district.16
HSAs program.
HSAs are community-based health workers recruited and salaried by the Malawi MOH. This cadre of worker was established for smallpox vaccination in the 1960s and continued to serve evolving needs of the health system, including response to cholera outbreaks during the 1970s and 1980s and environmental health education and population surveillance in the 1990s. With a grant from the Global Fund in 2008, the government doubled the size of the HSA workforce to over 10,000 HSAs, each serving approximately 1,000 people, for the delivery of community-based interventions. The minimum education level for HSAs is a junior certificate (grade 10), and all HSAs follow a 10-week basic training to learn the core set of tasks for which they are responsible (not including iCCM). Their remuneration is based on the government's civil service salary scale and equivalent to the remuneration of a first-level clerical staff. The current job description includes (1) promotion of hygiene and sanitation, (2) provision of health education, (3) home visitation and maintenance of community registers, (4) conducting community assessments, including public facility inspection, (5) disease surveillance, (6) conducting outreach clinics, including immunization, and (7) conducting VHCs to provide iCCM services. Additionally, selected HSAs are also involved in diverse activities, such as distribution and administration of contraception, treatment of tuberculosis, and voluntary counseling and testing for HIV. Many HSAs are young and male. They do not always originate from the communities that they serve and may not reside in their catchment area.
Introduction of iCCM in Malawi.
Caring for the sick child in the community.
The WHO/UNICEF training materials on caring for the sick child in the community are a simplified version of the IMCI guidelines for first-level health workers and focus on the major causes of death among children under age 5 years.17 CBHWs learn to identify and treat uncomplicated cases of suspected pneumonia, fever (presumed malaria), and diarrhea and identify and refer children with danger signs, severe malnutrition, or other problems that they have not been trained to treat. A job aid, known as the Sick Child Recording Form (SCRF), specifies the algorithms for assessment and classification of the sick child's signs and symptoms, and it guides CBHWs on selection of treatment with an antibiotic, antimalarial, and/or oral rehydration salt (ORS) and zinc tablet (Panel 1). The SCRF serves as the basis for training and can serve as a main reference tool when providing services in the community.

Sick child recording form job aid with iCCM guidelines.
Citation: The American Society of Tropical Medicine and Hygiene 87, 5_Suppl; 10.4269/ajtmh.2012.11-0759
{kind=link}
Provision of iCCM requires minimal medicines and equipment. In addition to the four essential medicines listed, CBHWs also learn to use a rapid diagnostic test (RDT) to assess for malaria and a mid-upper arm circumference (MUAC) strap to assess for severe acute malnutrition. A timer to count respiratory rate is desirable but not mandatory.
The initial iCCM training is 6 days and includes seven clinical practice sessions, two sessions in inpatient facilities to practice recognition of danger signs and five sessions in outpatient facilities to practice the entire process of assessment and treatment or referral. A follow-up visit to the CBHW by an experienced facilitator within 4–6 weeks of training is strongly recommended for additional skills reinforcement; also, regular supervision that includes observation of clinical practice is recommended.
Adoption and early introduction.
The Malawi MOH IMCI unit adopted the materials included in caring for the sick child in the community in June of 2008 after a demonstration course. Minimal adaptations were made to the clinical content (i.e., the inclusion of palmar pallor as a danger sign and management of eye infections). Use of RDT to assess for malaria was not part of the initial version of the WHO/UNICEF generic materials and hence, was not included in the adaptation. It was decided that the implementation strategy would target HSAs in hard-to-reach areas based on (1) distance to the nearest health facility of 8 km or more or (2) difficult access because of geographical terrain or natural barriers. Using these criteria, district management teams (DHMTs) identified 3,452 hard-to-reach areas.
Targeting the hard-to reach areas, DHMTs, under the guidance of the district IMCI coordinator, became responsible for establishing community-based child health services. Establishment involved conducting community orientation and HSA training, providing medicines and supplies, supervision, and monitoring. HSAs are provided a drug box after training, and they replenish medicines from the nearest health center. They use a register based on the SCRF to record the care provided to children that they see. They send standard reporting forms to the health facility monthly, from which summary reports are sent to the DHMT and the national IMCI unit. Village health committees support and safeguard the work of an HSA. For example, the committee contributes to managing the medicine supply by holding a key for the HSA's drug box; the drug box has double locks, and a committee member must assist the HSA in opening the box on the day of the VHC. HSAs, in principle, conduct VHCs to provide curative care on scheduled days of the week, taking into consideration their other responsibilities and tasks.
Early implementation of iCCM in Malawi.
Current implementation status.
By the end of 2010, all districts in Malawi had adopted the policy of iCCM, focusing on the establishment of VHCs by iCCM-trained HSAs in hard-to reach areas. As of September of 2011, 3,296 HSAs had received iCCM training, and 2,709 (or 79%) were providing services, hence managing functional VHCs. The iCCM approach was being implemented in all districts, with 13 of 28 districts having coverage of more than two HSAs per 10,000 total population (Figure 1A). All but 2 districts had reached 50% coverage of the targeted hard-to-reach areas, and 17 districts had reached coverage of 76% or more (Figure 1B).
District coverage of iCCM-trained HSAs (A) by population and (B) in hard-to-reach areas.
Citation: The American Society of Tropical Medicine and Hygiene 87, 5_Suppl; 10.4269/ajtmh.2012.11-0759
{kind=link}
Use of iCCM services and children treated for common illnesses.
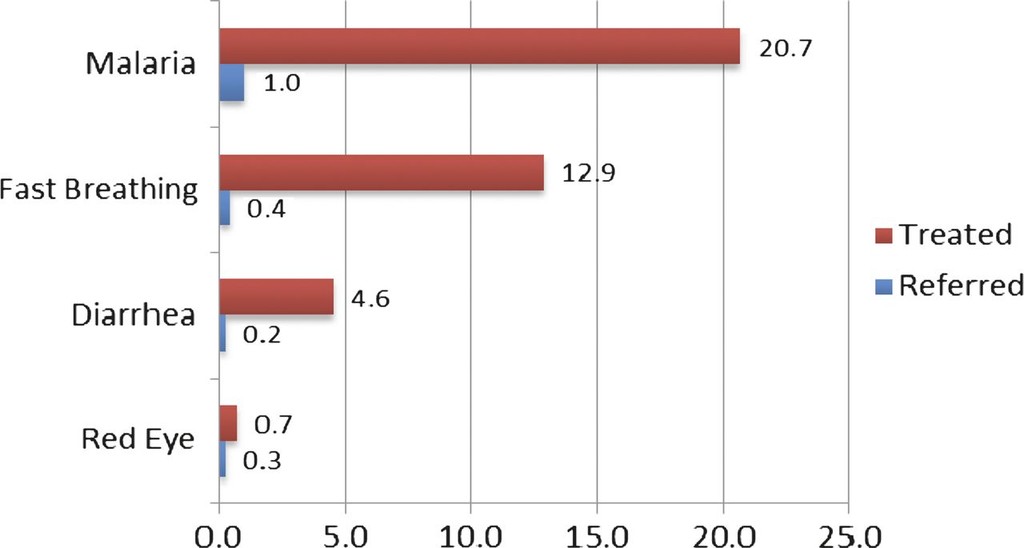
A quality of care assessment undertaken in 2009 (described below) included a review of HSA registers to assess routine use of iCCM services in six districts with early implementation.14 Of 131 HSAs surveyed, 102 HSAs had complete registers for the month of September of 2009 and had documented seeing a median number of 41 sick children per month (interquartile range of 19–73 visits per month). The central IMCI unit established a system to monitor use of iCCM services in 2009. For the period of October of 2010 to September of 2011, on average, 68% of functional VHCs submitted monthly reports. Figure 2 summarizes the numbers of treatments given and referrals made at those VHCs per 1,000 children ages 0–4 years in all districts. To reflect the national policy of VHCs in hard-to-reach areas, an analysis of the average monthly number of treatments by VHCs was also done for one district with a high level of monthly reporting by HSAs. Figure 3 shows the average monthly number of treatments and referrals at VHCs in Phalombe district in the period of January to December of 2011. Each VHC treated an average of 41.3 children for fever (presumed malaria), an average of 20.6 children for presumptive pneumonia, and an average of 11.6 children for diarrhea each month. On average, two children were referred every month. The predominance of fever treatments may be partially explained by the national policy of presumptive treatment of fever for malaria.
Monthly average number of treatments given and referrals made at VHCs per 1,000 population ages 0–4 years in all districts from October of 2010 to September of 2011.
Citation: The American Society of Tropical Medicine and Hygiene 87, 5_Suppl; 10.4269/ajtmh.2012.11-0759
{kind=link}
Monthly average number of treatments given and referrals made at VHCs in Phalombe district per health clinic from January to December of 2011.
Citation: The American Society of Tropical Medicine and Hygiene 87, 5_Suppl; 10.4269/ajtmh.2012.11-0759
{kind=link}
Selected quality of care findings.
In late 2009, IIP-JHU, MOH, and WHO conducted an early assessment of the quality of iCCM services provided in the community by HSAs; the full methodology and results are described elsewhere. Briefly, the assessment was carried out in six districts that had made progress in implementation as of September of 2009. Table 1 presents selected results from directly observed consultations with sick children for common illnesses (signs of pneumonia, fever/malaria, and diarrhea) and danger signs compared with a clinician trained as a master iCCM trainer. The proportion of sick children receiving correct assessment, classification, and treatment of common illnesses was similar to the proportion observed in previous studies.18,19 Just over one-half of children requiring referral were referred appropriately. An analysis of common errors in clinical steps reported elsewhere provides additional insight into the factors affecting the performance. For example, only 37% of children were assessed correctly for all four physical danger signs. The survey also assessed caregiver satisfaction through an exit interview, in which 97% of caregivers reported to have found the services excellent (34%) or good (63%) and 99% reported that they would visit the HSA again for a child's illness. Qualitative interviews indicated that both program managers and HSAs positively received the program.15 HSAs reported increased feelings of usefulness and respect in the community, although they also perceived their workload to have increased with iCCM.15
Selected results from the quality of care assessment of HSAs providing community case management services for common child illnesses in Malawi in October and November of 2009
| N (sick children) | In six districts (95% CI)* | |
|---|---|---|
| Sick child consultation for common illnesses | ||
| Proportion of children assessed for cough, fever, and diarrhea | 382 | 77% (71–82%) |
| Proportion of children with classifications matching fever, cough and fast breathing (pneumonia), and diarrhea | 382 | 68% (62–73%) |
| Proportion of children receiving correct treatment of fever, pneumonia,† and/or diarrhea | 242 | 62% (56–68%) |
| Sick child consultation for danger signs | ||
| Proportion of children assessed for four physical danger signs‡ | 382 | 37% (30–45%) |
| Proportion of children with danger signs requiring referral who were referred | 69 | 55% (42–68%) |
95% Confidence limit adjusted for sick children seen by the same HSA (within HSA correlation).
Defined as cough and fast breathing.
Chest indrawing, palmar pallor, red on MUAC tape, and swelling of both feet.
The assessment found that supervision and drug supply in the first year were less than optimal. Less than 40% of HSAs included in the sample had received an iCCM-specific supervisory visit in the previous 3 months, and only 16% received a visit that included clinical observation of case management. Although the sample was drawn only from HSAs having received initial drug stocks, only 69% of VHCs manned by HSAs had all three primary treatments (cotrimoxizole, antimalarials like lumefantrine-artemether [LA], and ORS) on the day of the visit.14
A telephone survey conducted by the Malawi NSO and IIP-JHU in coordination with the MOH between March and April of 2011 in the Balaka district found that, among 49 iCCM-trained HSAs, 74% had received a medicine box, 71% had treated sick children in the previous 3 months, and 67% had treated sick children in the previous 7 days. The proportion of HSAs with an uninterrupted stock in the previous 3 months was 11% for ORS, 40% for LA, and 82% for cotrimoxazole16; 53% of HSAs had received supervision in the previous 3 months, 29% of HSAs had supervision at their VHC, and 40% of HSAs reported receiving iCCM-specific supervision with reinforcement of clinical practices in the health center or at their VHC.16 Although this survey was restricted to one district in Malawi's central region, the high levels of CCM activity among trained HSAs who received their drug boxes are consistent with the use reports of Phalombe district included in Figure 2.
Discussion
After the first 3 years of implementation, the iCCM approach is showing signs of success in Malawi. First and foremost, there is strong MOH support for both the policy and practice of iCCM. The HSA cadre is quite stable and well-respected in the communities, both likely a result of the cadre being salaried and formally recognized by the MOH. Routine monitoring and survey data, albeit incomplete, show stable monthly use rates of HSAs' iCCM services and relatively high measured quality of care. Data from the most recent Demographic and Health Survey (DHS) show that care seeking for pneumonia and fever in a health facility or from a skilled provider were reported at 65.7%, and 59.4%, respectively. Care seeking for diarrhea and treatment with ORS were reported at 57.3% and 69%, respectively.20 These data suggest progress since 2006, when care seeking for pneumonia was reported at 51% and treatment of diarrhea was reported at 26%.
Although factors that have facilitated the scale up of the iCCM services to date can be identified (Table 2), there are also important challenges that affect the availability and quality of the community-based services. Several areas stand out.
Meeting the challenges of scaling up iCCM in Malawi
| Program component | What has been shown to work |
|---|---|
| National orientation and capacity building | Clear leadership of the MOH and an understanding of partners about their roles and responsibilities |
| Demonstration course for district and national managers to create awareness among relevant stakeholders | |
| National planning and adaptation workshop to reach consensus moving forward | |
| Minimal adaptation to the generic WHO/UNICEF guidelines | |
| Orientation of DHMTs, mapping of hard-to-reach areas, and joint planning | |
| Engagement of the national IMCI technical working group in the process | |
| Proper coordination of available support and collaboration of partners to roll out activities in assigned districts | |
| Community ownership and participation | Community dialogue before introduction of the services |
| Formation of village health committees under each functional VHC | |
| Engagement of community leaders to manage the VHC | |
| Skills building | Devolution of HSAs training to district level |
| Leadership of district IMCI coordinators and engagement of DHMT members | |
| Appropriate case load in district hospitals for inpatient and outpatient clinical practice during training | |
| Supervision | Assignment of specified responsibilities to various cadres of staff (senior HSA, environmental officer, and community nurse) |
| Training supervisors in iCCM and supervisory skills | |
| Development of integrated checklists incorporating key elements of the sick child recording form | |
| Creation of a mentorship program for periodic skills reinforcement of trained HSAs | |
| Medicines and supplies | Provision of medicines to HSAs during their monthly visits to the designated health center |
| Supervisors carrying medicines and supplies to alleviate stock outs | |
| Guidance on quantification of medicines to DHMTs | |
| Rollout of standard operating procedures for logistics management information systems to strengthen use and management of medicines and other supplies | |
| Referral | Designation of health centers where HSA should refer |
| Use of referral note and feedback on the same | |
| Engagement of VHC in finding solutions to facilitate referral, such as bicycles or ox cart as transport, and escorts at night | |
| Monitoring | Recruitment of a national monitoring and evaluation officer in the IMCI unit |
| Development of the iCCM register based on the sick child recording form | |
| Quality of care assessment of HSAs performance | |
| District-based village clinic review meetings to strengthen implementation | |
| Motivation | Recognition of HSAs as formal members of the health work force |
| Provision of adequate housing to HSAs in hard-to-reach areas through village health committees | |
| Innovations | Provision of mobile phones to HSAs to facilitate contact and SMS-based reporting and ordering of medicines and supplies |
The first area relates to the frequent stock outs of medicines. Limited district budgets and stock outs at health centers, where HSAs are supposed to restock their supplies, combined with limited capacity for forecasting needs have led to important breakdowns in service provision in the community. There are serious concerns that these disruptions will, in the long run, undermine the credibility of the HSAs and the likelihood that families will seek care promptly when children show signs of illness. To overcome this barrier, partners, such as Management Sciences for Health (MSH) and John Snow International (JSI), have been working with the MOH to strengthen logistics management, including forecasting and medicine quantification, to improve the consistency of drug supply to VHCs. The MOH is also piloting the introduction of RDTs for assessing children with fever, which will contribute to further rationalizing of the use of antimalarials. An initiative currently implemented in six districts is the Supply Chain Management for iCCM (SC4CCM) approach, which uses frontline Short Message Service (SMS) for monthly reporting and ordering of stocks by HSAs. The system connects each HSA with the supply manager in the DHMT who receives the SMS information, prepares the new supply, and notifies the HSA when it is ready for pick up in the health facility. The system is to be fully evaluated, but preliminary experiences suggest fewer stock outs among participating HSAs.
A second main challenge is that VHCs are scheduled in light of other responsibilities that the HSAs have to fulfill, and in some instances, they are conducted only one or two times per week. Hence, services may not be available when a child needs them. This concern seems to be less of an issue when the iCCM-trained HSA resides in the community, but it is a seriously limiting factor to service availability in communities that are served by HSAs who do not live in their catchment area. Although a stronger articulation of national policy on the provision of services in VHCs will be required, planning and management at the district level has proven to be an important factor in addressing this challenge. Verbal reports from IMCI coordinators and district health officers have indicated that community dialogue and engagement of the village health committees in planning and managing the community service have been critical for the initiation and sustainability of the services. Where communities were involved from the start, they took responsibility to establish housing for the HSAs, identified the location of the VHC, constructed the building, and assisted in managing the service, including monitoring of the drug box. In districts with little efforts to community involvement, DHMTs experienced difficulties in finding housing for trained HSAs in the targeted communities and initiating the VHC services. Anecdotal evidence suggests that, where HSAs reside in their community, access to iCCM extends beyond the VHC hours, and community members can consult the HSAs more frequently or on need.
A third challenge relates to the linkages between the HSAs and the health center level for timely referral, improved monitoring, and supervision. Although the results of the quality of care assessment of HSAs were encouraging, they also illustrated a clear need for skills reinforcement and sustained support. The fact almost one-half of children requiring referral were not appropriately referred is of particular concern, and this information calls for continued education and practice of assessment and decision-making skills, including through direct observation, vignettes, and photo and video exercises. Designated supervisors are senior HSAs and environmental health officers who traditionally do not have clinical responsibilities. They are trained in iCCM but do not treat sick children. To bridge the gap in their skills to provide effective supervision, the MOH, in collaboration with Save the Children, has developed a 2.5-day competency-based supervisory skills training course that targets the senior HSAs and environmental health officers. In addition, the MOH is promoting other skills reinforcement activities, such as mentoring of HSAs by clinical staff in health facilities. The fact that HSAs visit the health facility regularly provides a clear opportunity for organizing a program of work to strengthen the knowledge and skills of HSAs. However, it requires that the staff in health facilities is well-versed with the iCCM approach and can act as a gold standard for iCCM management. Results from a health facility survey among IMCI-trained health professionals also conducted in 2009 showed that quality of sick childcare in health facilities had important limitations and was not markedly better than the care in VHCs.21 Hence, the approach for quality improvement has to address HSAs and health facility-based staff in concert.
The MOH, in collaboration with the independent evaluation team at IIP-JHU and Malawi NSO, has embraced a national platform approach to evaluation of the iCCM program.22 In this approach, monitoring program implementation and outputs is an essential pre-requisite to attribute any changes in coverage and/or mortality to the CCM program. The MOH and partners are working to strengthen the availability and reliability of CCM indicators, many analogous to the proposed CCM Benchmark indicators,23 at the district level. An emphasis on better information at the district level through routine monitoring and special exercises, such as telephone surveys among iCCM-trained HSAs to assess drug supplies, frequency and content of supervision, and use of services,16 will provide additional information about the strength of CCM implementation and allow program managers to identify ongoing weaknesses for improvements.
In conclusion, although it is too early to determine the effects of introducing iCCM in Malawi on treatment coverage and under 5 years child mortality, the strategy has the potential to achieve the government's goal of universal coverage of key child health interventions. Moving curative services closer to communities can help to overcome important geographical barriers to accessing care for sick children. The MOH and its partners are researching and developing strategies to ensure ongoing quality of services and availability of drugs and commodities. Among other developments, the MOH may adapt the iCCM recording form to include RDTs of all children with fever to ascertain the likelihood of malaria. A policy discussion on the need for daily service delivery has also been initiated with a view on revision of this aspect in the job description of iCCM-trained HSAs. An ongoing prospective evaluation of MNCH rapid scale up in Malawi, which strongly focuses on the iCCM approach, will provide evidence if the rollout is related to increases in treatment coverage and decreases in mortality among children less than 5 years of age.
ACKNOWLEDGMENTS
The authors thank all individuals and partners who contributed to the introduction and scale up of the iCCM approach in Malawi, especially Dr. S. B. Kabuluzi, Edward Nkhono (MOH), Susan Kambale (WHO), Ketema Bizuneh (UNICEF), Rudi Thetard (USAID/BASICS), Robert Mahala (JSI), Tiyese Chimuna (Save the Children), Dyson Likomwa (Population Services International), and the staff responsible for scale up of MNCH interventions in the districts. Grants made available by the Bill and Melinda Gates Foundation (BMGF) through the WHO and JSI, the Canadian International Development Agency (CIDA) through UNICEF, PSI, and Save the Children, and USAID through MSH/BASICS and JSI greatly facilitated the implementation. The external evaluation activities are funded by the BMGF and CIDA. We would also like to thank IIP-JHU and the Malawi NSO for sharing their results related to iCCM implementation; this study was led by Elizabeth Hazel at IIP-JHU and Willie Kachaka at Malawi NSO, with funding support from CIDA through the Real-Time Tracking of Results Grant and BMGF through a grant to the Partnership for Maternal, Neonatal and Child Health. H.N., B.D., J.A.C.-K., and K.G. conceptualized the paper. H.N., B.D., and L.M. prepared the first draft of the manuscript. A.M., J.A.C.-K., and K.G. prepared the coverage data and contributed to the writing and interpretation of the findings. T.K. reviewed the paper and provided suggestions.
- 1.↑
UN Interagency Group for Child Mortality Estimates, 2011. Levels and Trends in Child Mortality. New York: UNICEF.
- 2.↑
UNICEF, 2011. Countdown to 2015 Decade Report (2000–2010): Tracking Stock of Maternal, Newborn and Child Survival. New York: UNICEF.
- 3.↑
WHO, 2005. World Health Report Making Every Mother and Child Count. Geneva, Switzerland: World Health Organization.
- 4.↑
WHO, UNICEF, 2004. Joint Statement on Management of Pneumonia in Community Settings. New York: UNICEF.
- 5.↑
UNICEF, 2012. Countdown to 2015: Tracking Progress in Maternal, Newborn and Child Survival. Progress Report 2012. New York: UNICEF.
- 6.↑
UNICEF, 2010. Community Case Management of Diarrhoea, Malaria and Pneumonia of Sick Children for Sub-Sahara Africa in 2010: Data Report of a Desk-Based Survey of UNICEF Country Offices. New York: UNICEF.
- 7.↑
Bhutta ZA, Lassi ZS, Parito G, Huicho L, 2010. Global Experience of Community Health Workers for Delivery of Health Related Millennium Development Goals: A Systematic Review, Country Case Studies, and Recommendations for Integration into National Health Systems. Geneva, Switzerland: Global Health Workforce Alliance.
- 8.↑
Haines A, Sanders D, Lehman U, Rowe AK, Lawn JE, Jan S, Walker DG, Bhutta Z, 2007. Achieving child survival goals: potential contribution of community health workers. Lancet 369: 2121–2131.
- 10.↑
UNICEF and Malawi National Statistics Office, 2008. Malawi Multiple Indicator Cluster Survey 2006. Final Report. Lilongwe, Malawi: UNICEF and Malawi National Statistics Office.
- 11.↑
Joint United Programme on HIV/AIDS, 2010. Malawi HIV, Monitoring AIDS, and Evaluation Report: 2008–2009. UNGASS Country Progress Report, 2010. Geneva, Switzerland: Joint United Programme on HIV/AIDS.
- 12.↑
Ministry of Health Malawi, 2004. A Joint Programme of Work for a Health Sector-Wide Approach (SWAP), 2004–2010. Lilongwe, Malawi: Government of Malawi.
- 13.↑
National Statistics Office, Malawi, 2008. Population and Housing Census Main Report. Available at: http://www.nso.malawi.net/. Accessed July 25, 2012.
- 14.↑
Gilroy KE, Callaghan-Koru JA, Cardemil CV, Nsona H, Amouzou A, Mtimuni A, Daelmans B, Mgalula L, Bryce J on behalf of the CCM-Malawi Quality of Care Working Group, 2012. Quality of sick child care delivered by Health Surveillance Assistants in Malawi. Health Policy Plan: first published online October 13, 2012. doi:10.1093/heapol/czs095.
- 15.↑
Callaghan-Koru JA, Hyder AA, George A, Gilroy KE, Nsona H, Mtimuni A, Bryce J, 2012. Health workers' and managers' perceptions of the integrated community case management program for childhood illness in Malawi: the importance of expanding access to child health services. Am J Trop Med Hyg 87 (Suppl 5): 61–68.
- 16.↑
National Statistical Office, Malawi, 2011. Institute for International Programs—Johns Hopkins University, USA Measuring CCM Implementation Strength Report of Findings from a Pilot of Study Catalytic Initiative Rapid Scale-Up Program, Malawi. Lilongwe, Malawi: Government of Malawi.
- 17.↑
WHO/UNICEF, 2011. Caring for the Sick Child in the Community. Geneva, Switzerland: World Health Organization.
- 18.↑
Kelly JM, Osamba B, Garg RM, Hamel MJ, Lewis JJ, Rowe SY, Rowe AK, Deming MS, 2001. Community health worker performance in the management of multiple childhood illnesses: Siaya District, Kenya, 1997—2001. Am J Public Health 91: 1617–1624.
- 19.↑
Rowe SY, Kelly JM, Olewe MA, Kleinbaum DG, McGowan JE, McFarland DA, Rochat R, Deming S, 2007. Effect of multiple interventions on community health workers' adherence to clinical guidelines in Siaya, Kenya. Trans R Soc Trop Med Hyg 101: 188–202.
- 20.↑
Ministry of Health Malawi, 2010. Demographic and Health Survey. Lilongwe, Malawi: Government of Malawi.
- 21.↑
Ministry of Health Malawi, 2009. Survey to Evaluate the Quality of Care Provided to Sick Children Attending a Health Facility. Lilongwe, Malawi: Government of Malawi.
- 22.↑
Victora CG, Black RE, Boerma JT, Bryce J, 2011. Measuring impact in the Millennium Development Goal era and beyond: a new approach for large-scale effectiveness evaluations. Lancet 377: 85–95.
- 23.↑
McGorman L, Marsh DR, Guenther T, Gilroy K, Barat LM, Hammamy D, Wansi E, Peterson S, Hamer DH, George A, 2012. A health systems approach to integrated community case management of childhood illness: methods and tools. Am J Trop Med Hyg 87 (Suppl 5): 69–76.