






{kind=link}
INTRODUCTION
Scrub typhus, a vector-borne rickettsiosis caused by Orientia tsutsugamushi infection, is one of the leading causes of non-malarial febrile illness in Asia. 1 The disease presents as acute undifferentiated fever with or without eschar. The clinical picture is characterized by fever with chills, myalgia, headache, abdominal pain, vomiting, and capillary leak during the first week of illness. Its nonspecific clinical features and shared seasonal profile with dengue and leptospirosis hamper its early diagnosis, particularly in the tropics. 2 The pathophysiology is not entirely clear, though in general, it is assumed to be disseminated vasculitis with primary target being vascular endothelium. Complex interplay of host and pathogen response with combined humoral and cellular immunity contributes to the development of vascular injury to skin, lungs, liver, and brain. 3 The gold standard test for diagnosis, the indirect immunofluorescent assay, is prohibited by exorbitant cost and the need for personnel trained in fluorescent microscopy and is usually limited to research centers. 4 Laboratory confirmation, in resource-constrained settings, is commonly accomplished by IgM ELISA (InBios International Kit), with 91% sensitivity and 99% specificity. 5–7 The disease, in general, portends a mild phenotype with a median mortality of 6% (0–70%) if left untreated. 8 Complications of scrub typhus are organ-specific and comprise acute respiratory distress syndrome, acute kidney injury, myocarditis, meningoencephalitis, and disseminated intravascular coagulation. 9,10 Given the poorly defined symptomatology and life-threatening complications if left untreated, early diagnosis and judicious antibiotic therapy with tetracyclines/chloramphenicol is crucial. The research objective was to study the clinical profile of children with scrub typhus diagnosed by IgM ELISA admitted at a tertiary care teaching institute in South India with special reference to the myriad of typical and atypical manifestations.
METHODOLOGY
This study is a retrospective review of children with clinical and laboratory diagnosis of scrub typhus presenting to the Department of Paediatrics, Pondicherry Institute of Medical Sciences, a tertiary care teaching institute in South India, during the period of January 2012–December 2018. Children younger than 12 years presenting with acute undifferentiated fever, defined as acute febrile illness with onset in the previous 2 weeks with fever of > 38°C for at least 48-hour duration, were screened for eligibility. Children with seropositive IgM ELISA for scrub typhus were enrolled in the study. The InBios International Kit with a sensitivity of 91% and a specificity of 99% was used for diagnostic testing. A sample absorbance value > 0.5 was established as the cutoff criteria based on the local healthy normal sera. Children with classical symptoms and signs suggestive or diagnostic of a particular febrile illness (other than scrub typhus) or with chronic or recurrent febrile illness were excluded. Children with objective evidence of organ dysfunction such as myocarditis, meningoencephalitis, pneumonia, acute kidney injury, acute respiratory distress syndrome, disseminated intravascular coagulation, pancreatitis, and hemophagocytic lymphohistiocytosis were considered as severe scrub typhus. The study was approved by the Institutional Ethics Committee (IEC-RC/16/147). Waiver of parental consent was obtained from the Institutional Ethics committee because this was a retrospective chart review. Clinical features, laboratory investigations, treatment received, and the outcome recorded were obtained. The data were entered in a data recording form and then transcribed to MS Excel data and analyzed using SPSS Statistics for Windows, Version 17.0 (SPSS Inc., Chicago, IL). Descriptive data were represented by frequency, percentage, and mean ± SD. The chi-square test for dichotomous variables and t test and Mann–Whitney U test for continuous variables were applied. The associations of clinical and laboratory variables were studied by multivariate regression and logistic regression. P < 0.05 was considered statistically significant.
RESULTS
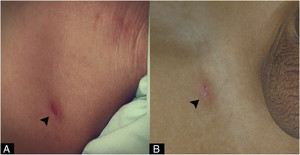
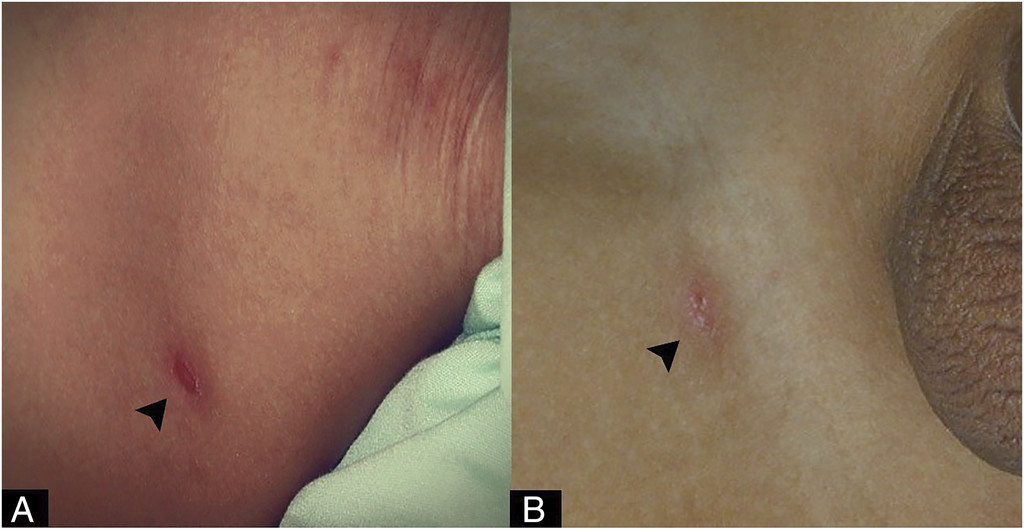
During the period of January 2012–December 2018, records of 41,365 children presenting to the pediatric services with fever were reviewed, and a total of 262 children with undifferentiated fever and IgM ELISA positivity for scrub typhus were diagnosed. Of these, 170 were boys (65%) and more than half of the children were between the age-group of 1–5 years (Table 1). The youngest infant diagnosed was aged 5 months, and 13 children (5%) presented during infancy. Fever was universal, and 128 children presented within the first 5 days of fever (44%). Generalized lymphadenopathy (93.5%) and hepatomegaly (70%) were the most common clinical findings. Painless eschar was identified in 31% of children, with greater predilection for groin and axilla (Figure 1). Nineteen children had developed a diffuse maculopapular rash. The laboratory profile of children with scrub typhus is illustrated in Table 2. Thrombocytopenia defined by a platelet count of less than 100 × 109/L of blood was striking in one-third of children. Of the 262 children, 25 children were found to have severe scrub typhus and 18 children required intensive care stay; nine required ventilator support for pneumonia, and six required neurocritical care monitoring for meningoencephalitis. Chest radiograph suggestive of bronchopneumonia was noted in 11 children, and hemophagocytic lymphohistiocytosis was identified in three children (Table 3). There was no mortality during the study period. Multivariate analysis revealed elevated aspartate aminotransferase as a significant predictor of severity of scrub typhus ([OR 3.9], P value 0.005). Other variables such as fever > 5 days, eschar, leukocytosis, thrombocytopenia, hypoalbuminemia, and hyponatremia were insignificant. Overall, 239 children received doxycycline therapy, and 23 received azithromycin therapy. Severe forms of scrub typhus with complications received a 14-day therapy. Rapid defervescence within 48 hours was noted in 87% of the children. Table 4 compares the profile of children based on eschar, a clinical hallmark of scrub typhus. Clinical evidence of lymphadenopathy was found to have a significant association with eschar in children with scrub typhus (P < 0.005).
Clinical characteristics of 262 children with scrub typhus infection
| Characteristic | Number | Percentage | |
|---|---|---|---|
| Gender distribution | Male | 170 | 64.9 |
| Female | 62 | 23 0.6 | |
| Age distribution (years) | < 1 | 13 | 4.9 |
| 1–5 | 152 | 58.1 | |
| 6–10 | 82 | 31.29 | |
| 11–14 | 15 | 5.7 | |
| Duration of fever (days) | < 3 | 19 | 7.2 |
| 3–5 | 99 | 37.7 | |
| > 5 | 144 | 54.9 | |
| Vomiting | 79 | 30.2 | |
| Abdominal pain | 33 | 12 | |
| Maculopapular rash | 19 | 7.2 | |
| Generalized edema | 37 | 14.12 | |
| Respiratory distress | 12 | 4.5 | |
| Lymphadenopathy | 245 | 93.5 | |
| Generalized | 217 | 82 | |
| Localized | 28 | 10.6 | |
| Eschar | 83 | 31.6 | |
| Interscapular area | 4 | 4.8 | |
| Wrist | 1 | 1.2 | |
| Leg | 11 | 13.25 | |
| Axilla | 19 | 22.8 | |
| Groin | 20 | 24.09 | |
| Ear lobe | 6 | 7.22 | |
| Trunk | 8 | 9.6 | |
| Neck | 8 | 9.6 | |
| Shoulder | 2 | 2.4 | |
| Eyelid | 4 | 4.8 | |
| Jaundice | 1 | 0.3 | |
| Hepatomegaly | 185 | 70 | |
| Hepatosplenomegaly | 87 | 33.2 | |
| Encephalopathy | 6 | 2.3 | |

Well-established eschar in the axilla (A) and groin (B).
Citation: The American Journal of Tropical Medicine and Hygiene 104, 2; 10.4269/ajtmh.20-1019
Laboratory profile of 262 children with scrub typhus infection
| Laboratory parameter | Cutoff | Number | Percentage |
|---|---|---|---|
| Thrombocytopenia (×109/L) | < 100 | 83 | 31.6 |
| < 50 | 10 | 12 | |
| > 50 | 73 | 87 | |
| Total leukocyte count (mL) | < 4,000 | 48 | 18.3 |
| 4,000–11,000 | 169 | 64.5 | |
| > 11,000 | 45 | 17.1 | |
| Anemia | 76 | 29 | |
| < 1 years | 3 | 3.6 | |
| 1–5 years | 40 | 53.2 | |
| 5–10 years | 27 | 35.3 | |
| > 11 years | 6 | 7.9 | |
| Raised liver enzymes (> 120 IU/L) | AST | 69 | 26 |
| ALT | 47 | 18 | |
| Hyponatremia | < 135 meq/L | 43 | 16.5 |
| Hypoalbuminemia | < 3.5 g/dL | 39 | 14.8 |
| Erythrocyte sedimentation rate | > 30 mm/hour | 23 | 8.7 |
| Total bilirubin | > 2 mg/dL | 1 | 0.3 |
| Chest X-ray | Bronchopneumonia | 11 | 4.1 |
| Echocardiography | Left ventricular dysfunction | 1 | 0.3 |
| Neuroimaging | Contrast enhancement | 3 | 1 |
| IgM ELISA scrub typhus | > 0.5 OD | 262 | 100 |
AST = aspartate aminotransferase; ALT = alanine aminotransferase; OD = optical density; IU/L = international units per litre.
Clinical profile of 25 children with severe form of scrub typhus infection
| Characteristic | Number | Percentage | |
|---|---|---|---|
| Median age, years (IQR) | 4 (1–9) | ||
| Male | 15 | 60 | |
| Duration of fever (days) | < 3 | 4 | 16 |
| 3–5 | 7 | 28 | |
| > 5 | 14 | 56 | |
| Median duration of fever, days (IQR) | 7 (3.5–7.5) | ||
| Complications | |||
| Bronchopneumonia | 11 | 4 | |
| Acute respiratory distress syndrome | 2 | 0.7 | |
| Meningoencephalitis | 6 | 2.3 | |
| Acute kidney injury | 2 | 0.7 | |
| Hemophagocytic lymphohistiocytosis | 3 | 1 | |
| Myocarditis | 1 | 0.3 | |
IQR = interquartile range.
Comparison of clinical and laboratory profile of children with scrub typhus based on eschar positivity
| Parameter | Eschar present (N = 83) | Eschar absent (N = 179) | P-value |
|---|---|---|---|
| Mean age (years) | 5 | 5 | |
| Gender | |||
| Male | 47 (56.6%) | 123 (68.7%) | 0.077 |
| Female | 36 (43.3%) | 56 (31.2%) | |
| Clinical profile | |||
| Fever < 5 days | 30 (36.1%) | 88 (49.1%) | 0.066 |
| Fever > 5 days | 53 (63.8%) | 91 (50.8%) | |
| Vomiting | 25 (30.1%) | 54 (30.1%) | 0.792 |
| Abdominal pain | 6 (7.2%) | 27 (15%) | 0.877 |
| Jaundice | 1 (1.2%) | 0 | – |
| Maculopapular rash | 12 (14.4%) | 7 (3.9%) | 0.95 |
| Edema | 22 (26.5%) | 15 (8.3%) | 0.061 |
| Respiratory distress | 3 (3.6%) | 9 (5%) | 0.088 |
| Encephalopathy | 3 (3.6%) | 3 (1.67%) | 0.796 |
| Lymphadenopathy | 82 (98.7%) | 163 (91%) | 0.0381 |
| Hepatomegaly | 63 (75.9%) | 122 (68.1%) | 0.253 |
| Splenomegaly | 34 (40.9%) | 53 (29.6%) | 0.095 |
| Laboratory profile | |||
| Anemia | 27 (32.5%) | 49 (27.3%) | 0.473 |
| Leukopenia | 14 (31.3%) | 34 (25.6%) | 0.416 |
| Thrombocytopenia | 31 (37.3%) | 52 (29%) | 0.229 |
| Raised AST | 25 (30.1%) | 44 (24.5%) | 0.419 |
| Raised ALT | 15 (18%) | 32 (18%) | 0.512 |
| Hyponatremia | 17 (20%) | 26 (14.5%) | 0.452 |
| Hypoalbuminemia | 16 (19%) | 23 (13%) | 0.482 |
| Raised ESR | 7 (8.4%) | 16 (9%) | 0.687 |
AST = aspartate aminotransferase; ALT = alanine aminotransferase; ESR = erythrocyte sedimentation rate.
DISCUSSION
In this 6-year retrospective study, the authors describe the profile of pediatric scrub typhus and share the single-center experience of one of the largest data in children from Indian subcontinent. IgM ELISA was used for the diagnosis of scrub typhus in our study. Weil Felix is the cheapest and the most easily available method for scrub typhus serological diagnosis and has been used hitherto in several studies. Its low sensitivity, dubious false positivity in Proteus infections and its utility only in the second week of illness are the major drawbacks and have been supplanted by other serological methods such as IgM ELISA, PCR, and indirect immunofluorescence assay. Indirect immunofluorescence assay is the gold standard test for diagnosis but is limited by expensive fluorescent microscopy and expert training. 4 IgM ELISA testing with optimal sensitivity (91%) and specificity (99%), like in our study, is the practical alternative in resource-limited settings. 7
In our study, boys and children younger than 5 years were likely to be infected with scrub typhus, similar to that reported by Ganesh et al. 11 This could be justified by the increased outdoor play in the vector-ridden vegetation by children. In addition, 13 infants (5%) were diagnosed with scrub typhus. This is in consonance with studies by Dinesh et al. and Palanivel et al. who had described infantile onset scrub typhus in approximately 10% of their cohorts. 12,13 This comparatively higher percentage reported by the two authors might be due to the less number of children recruited in their study. Given the restricted outdoor activity in infants, Narayanasamy et al. 13 suggested the role of mite-ridden rodents or domesticated dogs in the transmission. However, a secondary route of exposure with mites hidden in garments brought in from outdoors is a reasonable explanation. 14
Scrub typhus infection is the leading treatable cause of non-malarial febrile illness in Asia. Over the last decade, it has become a seemingly ubiquitous part of Indian subcontinent with several published reports from distinct geographical locations. A review of the published literature on pediatric scrub typhus from India over the last decade was carried out by the authors 11–21 (Table 5). For the purpose of this review, citations were identified through PubMed search limited to the past 10 years (2010–2019) using the search terms (including variations), “scrub typhus,” “children,” and “India,” combined with study filters for cohort studies and original research. Acute undifferentiated fever lasting for more than 5 days with hepatomegaly and lymphadenopathy is one of the compatible clinical features of scrub typhus infection and has been reiterated from our analysis. However, in areas of high endemicity such as India, the threshold for diagnosis has to be lowered, as exemplified from our study, where 44% of children were identified within the first 5 days.
Analysis of the clinical profile and outcome of pediatric scrub typhus infection from India during 2010–2019
| Rashna 15 | Palanivel 12 | Manish 18 | Krishna 16 | Kalal 19 | Bhat 20 | Dinesh 13 | Masand 21 | Ganesh 11 | Basu 14 | Bal 17 | Our study | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample size | 24 | 67 | 35 | 52 | 53 | 66 | 117 | 30 | 358 | 61 | 201 | 262 |
| Place of study | Shillong | Chennai | Pondicherry | Chennai | Bengaluru | Dehradun | Pondicherry | Rajasthan | Chennai | Kolkata | Odisha | Pondicherry |
| Year of publication | 2011 | 2012 | 2012 | 2015 | 2016 | 2016 | 2016 | 2016 | 2018 | 2019 | 2019 | 2020 |
| Mean age (years) | 9.4 | NA | 6.3 | NA | 7.3 | 8.8 | 6.5 | 8.5 | NA | 6 | 5.4 | 5 years |
| Age range | NA | 2m-NA | 1.5–12 | 7m-16 | NA | 8m-18 | 6m-12 | 3–16 | 1d-18 | 1.5–12 | NA | 7 m-12 |
| Male (%) | 54 | 44 | 60 | 57 | 71 | 59 | 50 | 70 | 59 | 53 | 62 | 65 |
| Fever > 5 days (%) | 100 | NA | 83 | 96 | NA | > 73 | 100 | 82 | 100 | 100 | 100 | 55 |
| Eschar (%) | 42 | 46 | 11 | 67 | NA | 20 | 42 | 3 | 67 | 49 | 18 | 32 |
| Hepatomegaly (%) | 33 | 98 | 91 | 94 | 67 | 82 | 70 | NA | 94 | NA | NA | 70 |
| Splenomegaly (%) | 46 | 88 | 60 | 73 | 32 | 59 | 54 | NA | 90 | NA | NA | 40 |
| Lymphadenopathy (%) | 12.5 | 60 | 37 | 15 | 49 | 38 | 35 | NA | 25 | 59 | 74 | 93.5 |
| Hepatosplenomegaly (%) | NA | NA | NA | NA | NA | NA | NA | 60 | NA | 52 | 33 | 33 |
| Edema (%) | NA | 52 | 60 | 50 | 24.5 | 39 | 21 | NA | 48 | 52 | 22 | 14 |
| Encephalopathy (%) | 17 | 58 | 23 | 7 | 17 | 23 | 25 | NA | NA | 34 | NA | 2.3 |
| Laboratory diagnosis | WF | ELISA | WF | ELISA | ELISA | ELISA | ELISA | ELISA | ELISA | WF/ELISA | ELISA | ELISA |
| Anemia (%) | NA | 83 | NA | NA | 70 | 62 | 56 | 60 | NA | 83 | 54 | 29 |
| Thrombocytopenia (%) | 26 | 78 | 31 | 25 | 66 | 53 | 16 | 26 | 23 | 59 | 43 | 32 |
| Hyponatremia (%) | 66 | 12 | 17 | 46 | 9 | NA | 40 | 10 | 35.5 | 50 | NA | 16.5 |
| Transaminitis (%) | 58 | 65 | 31 | 62 | 81 | 61 | 48 | 60 | 38 | 30 | 73 | 44 |
| Complications (%) | 66 | 70 | 94 | 15 | 56 | 83 | 43 | 13 | 14.5 | 17 | 5.5 | 9.5 |
| Mortality (%) | 0 | 18 | 3 | 0 | 0 | 7.5 | NA | 6.6 | 0.8 | 1.6 | 0 | 0 |
NA = not available; WF = Weil Felix.
Although eschar is indicative of scrub typhus infection, its absence does not rule out the disease. The prevalence of eschar is extremely variable, ranging from < 1 to 92% in the available literature. 22–24 It was noted in 31% of the children in our study. Eschar is highly evolving and develops at the site of mite bite; it initially begins as a central vesicle with surrounding erythema and overlaying scales and finally heals as necrotic lesion resembling a burn of a cigarette toward the end of the first week. 25 Dark skin tone, uncharacteristic manifestations of eschar, and concealed areas of the body like groin, axillary skin folds, and behind ear lobule are few of the challenges in clinical examination. We compared the clinical features of children with scrub typhus based on the eschar and found a significant association between clinical evidence of lymphadenopathy and eschar positivity. Accordingly, lymphadenopathy may be considered as a clinical pointer toward eschar, and a detailed serial examination is warranted. Also, clinical identification of eschar has diagnostic implications: PCR testing of the eschar swabbing is a rapid and reliable bedside tool in the early phase of the disease. 26,27
Scrub typhus is, in general, a simple febrile illness with admirable outcome if treated early, as evidenced by nil mortality in our 262 children. This is in concordance with previous studies from India where mortality rates predominantly ranged from 0% to 7.5%. Furthermore, only 25 children (9.5%) from our study developed severe forms of scrub typhus marked by organ dysfunction. This is remarkably low when compared with earlier studies from the same region. Manish et al. 18 demonstrated an exceedingly high complication rate following scrub typhus infection with high incidences of myocarditis (34%) and acute kidney injury (20%) in their cohort of 35 children.Rarity of the disease in the region, which is not a hilly area, low index of suspicion for early diagnosis in 2011 when the study was conducted, and their small sample size can explain the high complication rate noted by Manish et al. Our results, however, are comparable with the study of 358 children from Chennai, 150 km from our center, by Ganesh et al. 11 who reported a 14.5% complication rate. Furthermore, Ganesh et al. identified elevated aspartate aminotransferase liver enzyme levels and thrombocytopenia as predictors of complication due to scrub typhus. An elevated aspartate aminotransferase liver enzyme level as a determinant of severe scrub typhus has been re-established by our study. Intrahepatic sinusoidal endothelial vasculitis and direct cytopathic liver damage contribute to this elevation. Unexplained transaminitis without jaundice in a febrile child should raise the suspicion for scrub typhus infection in endemic areas. 28 Other predictors of severe scrub typhus such as hypoalbuminemia, hyponatremia, encephalopathy, and leukocytosis proposed by Naryananasamy et al. 29 were not recognized in our study.
Likewise, three children developed hemophagocytic lymphohistiocytosis following scrub typhus in our cohort. Pancytopenia and hyperferritinemia hinted at the diagnosis and intravenous azithromycin without chemotherapy was effective. Data on hemophagocytic lymphohistiocytosis, as a life-threatening complication of scrub typhus in children, are grossly deficient and limited to occasional case series. Jin et al. 30 reported the beneficial outcome in 15 children with scrub typhus associated HLH with intravenous antibiotics (azithromycin or chloramphenicol) without the need for 2004 HLH protocol chemotherapy.
Large sample size, robust back up of data from a single center, and analysis of predictors of severe scrub typhus are the strengths of the study. Our study has few limitations such as its retrospective design and evaluation of only hospitalized children with modest representation of the community.
In conclusion, our study accentuates the varied spectrum of tsutsugamushi infection in children including a 9.5% complication rate. Elevated aspartate aminotransferase enzyme levels is a predictor of severity. Meticulous examination for eschar is merited in children with lymphadenopathy. Zero mortality in our cohort signifies the excellent outcome with judicious first-line antibiotics.
ACKNOWLEDGMENT
The American Society of Tropical Medicine and Hygiene (ASTMH) assisted with publication expenses.
REFERENCES
- 1.↑
Bonell A , Lubell Y , Newton PN , Crump JA , Paris DH , 2017. Estimating the burden of scrub typhus: a systematic review. PLoS Negl Trop Dis 11: e0005838.
- 2.↑
Acestor N , Cooksey R , Newton PN , Ménard D , Guerin PJ , Nakagawa J , Christophel E , González IJ , Bell D , 2012. Mapping the aetiology of non-malarial febrile illness in Southeast Asia through a systematic review--terra incognita impairing treatment policies. PLoS One 7: e44269.
- 3.↑
Rajapakse S , Rodrigo C , Fernando D , 2012. Scrub typhus: pathophysiology, clinical manifestations and prognosis. Asian Pac J Trop Med 5: 261–264.
- 4.↑
Koh GCKW , Maude RJ , Paris DH , Newton PN , Blacksell SD , 2010. Diagnosis of scrub typhus. Am J Trop Med Hyg 82: 368–370.
- 5.↑
Blacksell SD , Tanganuchitcharnchai A , Nawtaisong P , Kantipong P , Laongnualpanich A , Day NPJ , Paris DH , 2016. Diagnostic accuracy of the InBios scrub typhus detect enzyme-linked immunoassay for the detection of IgM antibodies in northern Thailand. Clin Vaccin Immunol 23: 148–154.
- 6.
Blacksell SD , Jenjaroen K , Phetsouvanh R , Wuthiekanun V , Day NPJ , Newton PN , Ching WM , 2010. Accuracy of AccessBio immunoglobulin M and total antibody rapid immunochromatographic assays for the diagnosis of acute scrub typhus infection. Clin Vaccin Immunol 17: 263–266.
- 7.↑
Pote K , Narang R , Deshmukh P , 2018. Diagnostic performance of serological tests to detect antibodies against acute scrub typhus infection in central India. Indian J Med Microbiol 36: 108–112.
- 8.↑
Taylor AJ , Paris DH , Newton PN , 2015. A systematic review of mortality from untreated scrub typhus (Orientia tsutsugamushi). PLoS Negl Trop Dis 9: e0003971.
- 9.↑
Rajapakse S , Weeratunga P , Sivayoganathan S , Fernando SD , 2017. Clinical manifestations of scrub typhus. Trans R Soc Trop Med Hyg 111: 43–54.
- 10.↑
Luce-Fedrow A , Lehman ML , Kelly DJ , Mullins K , Maina AN , Stewart RL , Ge H , John HS , Jiang J , Richards AL , 2018. A review of scrub typhus (Orientia tsutsugamushi and related organisms): then, now, and tomorrow. Trop Med Infect Dis 3: 8.
- 11.↑
Ganesh R , Suresh N , Pratyusha LL , Janakiraman L , Manickam M , Andal A , 2018. Clinical profile and outcome of children with scrub typhus from Chennai, South India. Eur J Pediatr 177: 887–890.
- 12.↑
Palanivel S , Nedunchelian K , Poovazhagi V , Raghunadan R , Ramachandran P , 2012. Clinical profile of scrub typhus in children. Indian J Pediatr 79: 1459–1462.
- 13.↑
Narayanasamy DK , Arunagirinathan AK , Kumar RK , Raghavendran VD , 2016. Clinico - laboratory profile of scrub typhus–an emerging rickettsiosis in India. Indian J Pediatr 83: 1392–1397.
- 14.↑
Basu S , Saha A , Sarkar S , Sinha MK , Das MK , Datta R , Hazra A , Datta Kanjilal S , Datta S , 2019. Clinical profile and therapeutic response of scrub typhus in children: a recent trend from eastern India. J Trop Pediatr 65: 139–146.
- 15.↑
Dass R , Deka NM , Duwarah SG , Barman H , Hoque R , Mili D , Barthakur D , 2011. Characteristics of pediatric scrub typhus during an outbreak in the North Eastern region of India: peculiarities in clinical presentation, laboratory findings and complications. Indian J Pediatr 78: 1365–1370.
- 16.↑
Krishna MR , Vasuki B , Nagaraju K , 2015. Scrub typhus: audit of an outbreak. Indian J Pediatr 82: 537–540.
- 17.↑
Bal M , Mohanta MP , Sahu S , Dwibedi B , Pati S , Ranjit M , 2019. Profile of pediatric scrub typhus in odisha, India. Indian Pediatr 56: 304–306.
- 18.↑
Kumar M , Krishnamurthy S , Delhikumar CG , Narayanan P , Biswal N , Srinivasan S , 2012. Scrub typhus in children at a tertiary hospital in southern India: clinical profile and complications. J Infect Public Health 5: 82–88.
- 19.↑
Kalal BS , Puranik P , Nagaraj S , Rego S , Shet A , 2016. Scrub typhus and spotted fever among hospitalised children in South India: clinical profile and serological epidemiology. Indian J Med Microbiol 34: 293–298.
- 20.↑
Kumar Bhat N , Dhar M , Mittal G , Shirazi N , Rawat A , Prakash Kalra B , Chandar V , Ahmad S , 2014. Scrub typhus in children at a tertiary hospital in north India: clinical profile and complications. Iran J Pediatr 24: 387–392.
- 21.↑
Masand R , Yadav R , Purohit A , Tomar BS , 2016. Scrub typhus in rural Rajasthan and a review of other Indian studies. Paediatr Int Child Health 36: 148–153.
- 22.↑
Silpapojakul K , Chupuppakarn S , Yuthasompob S , Varachit B , Chaipak D , Borkerd T , Silpapojakul K , 1991. Scrub and murine typhus in children with obscure fever in the tropics. Pediatr Infect Dis J 10: 200–203.
- 23.
Sirisanthana V , Puthanakit T , Sirisanthana T , 2003. Epidemiologic, clinical and laboratory features of scrub typhus in thirty Thai children. Pediatr Infect Dis J 22: 341–345.
- 24.↑
Kim DM et al. 2007. Distribution of eschars on the body of scrub typhus patients: a prospective study. Am J Trop Med Hyg 76: 806–809.
- 25.↑
Park J , Woo SH , Lee CS , 2016. Evolution of eschar in scrub typhus. Am J Trop Med Hyg 95: 1223–1224.
- 26.↑
Le Viet N , Laroche M , Thi Pham HL , Viet NL , Mediannikov O , Raoult D , Parola P , 2017. Use of eschar swabbing for the molecular diagnosis and genotyping of Orientia tsutsugamushi causing scrub typhus in Quang Nam province, Vietnam. PLoS Negl Trop Dis 11: e0005397.
- 27.↑
Kim DM , Kim HL , Park CY , Yang TY , Lee JH , Yang JT , Shim SK , Lee SH , 2006. Clinical usefulness of eschar polymerase chain reaction for the diagnosis of scrub typhus: a prospective study. Clin Infect Dis 43: 1296–1300.
- 28.↑
Hu ML et al. 2005. Short report: abnormal liver function in scrub typhus. Am J Trop Med Hyg 73: 667–668.
- 29.↑
Narayanasamy DK , Arun Babu T , Vijayadevagaran V , Kittu D , Ananthakrishnan S , 2018. Predictors of severity in pediatric scrub typhus. Indian J Pediatr 85: 613–617.
- 30.↑
Jin YM , Liang DS , Huang AR , Zhou AH , 2019. Clinical characteristics and effective treatments of scrub typhus-associated hemophagocytic lymphohistiocytosis in children. J Adv Res 15: 111–116.