









{kind=link}
{kind=link}
{kind=link}
INTRODUCTION
Rocky Mountain spotted fever (RMSF) is a severe and potentially fatal tick-borne disease caused by infection with Rickettsia rickettsii, which is transmitted by several species of ticks of the genus Dermacentor (Dermacentor variabilis and Dermacentor andersoni), Rhipicephalus (Rhipicephalus sanguineus), and Amblyomma (Amblyomma cajennense, Amblyomma aureolatum, Amblyomma imitator, and Amblyomma sculptum). 1 Since the 1940s, R. sanguineus (the brown dog tick) has been considered the main vector responsible for transmitting R. rickettsii in Mexico, whereas D. variabilis and D. andersoni were considered the primary vectors in the United States. Beginning in the early 2000s, R. sanguineus has emerged as an important vector in southwestern United States as well. 2–4
Rhipicephalus sanguineus is capable of infesting dogs in high numbers and can feed on canines at all stages in the life cycle. Each life cycle stage is also capable of transmitting R. rickettsii. 5–7 Because of these features, many of the current outbreaks have occurred in communities with large populations of stray or free-roaming dogs. 7 Rhipicephalus sanguineus–transmitted RMSF is now prominent in both northern Mexico and the southwestern United States and reported year-round, although several environmental and climate factors may be related to its occurrence. 1,8,9
The initial stages of RMSF can be difficult to distinguish clinically from other febrile illnesses as symptoms include fever, chills, malaise, and myalgia. The initial days of illness are characterized by abrupt onset of high fever and can progress to include rash, respiratory distress, abdominal pain, coagulopathy, altered mental status, and shock in as few as 5 days if not treated promptly. 10,11 A rash is seen in 90% of patients and typically develops between days 2 and 4 of illness; late onset rash is associated with increased mortality because of delay in treatment. 12–15 Doxycycline is the treatment of choice for all age-groups, and recent studies have shown that doxycycline does not cause tooth staining in pediatric populations. 1,16,17
After decades of quiescence, RMSF re-emerged in northern Mexico, a historically endemic region, in the early 2000s. 18,19 Sonora is one of the most impacted states in northern Mexico, with 1,394 cases reported during the period 2003–2016, and a historic case fatality rate (CFR) of 18%. 20 In 2015, because of an increase in cases and deaths in several states of northern Mexico, El Centro Nacional de Programas Preventivos y Control de Enfermedades (CENAPRECE) of the Mexican Ministry of Health (MOH) issued a declaration of epidemiologic emergency for RMSF, which was updated in 2018. 21 In response to the growing case counts and high CFR, Sonora began an enhanced epidemiologic surveillance program to collect comprehensive information on clinical presentation, treatment, and diagnosis of RMSF in the state. We summarized the data to better understand the emergence, changing trends, and reasons for the high mortality rates associated with RMSF in northern Mexico.
MATERIALS AND METHODS
Data collection.
We conducted a retrospective review of all cases of RMSF reported to the Dirección General de Promoción a la Salud y Prevención de Enfermedades (DGPROSPE) during January 2015–December 2018. Providers completed the National Surveillance Case Report Form at the time of initial contact and collected data including demographics, exposure, and detailed clinical information. In the event, a patient was unable to provide information; the reporting providers completed the information to the best of their ability, typically with the assistance of a family member or accompanying relative. Additional laboratory, treatment, and outcome data were added retrospectively through epidemiologic follow-up. We analyzed all raw data from the Epidemiological Surveillance System for Rickettsial Diseases from the Sonora MOH. Geographic coordinates of cases were available and incorporated into the analysis. To calculate incidence rates, we used the most recently available National Institute of Geography and Statistics census data from 2010. The Sonora MOH has classified the state into six health jurisdictions: Hermosillo (1) is located centrally; Caborca (2), Santa Ana (3), and San Luis Rio Colorado (6) are in the north; and Ciudad Obregon (4) and Navojoa (5) are located in the southern portion of the state. Case fatality rates were calculated for each jurisdiction. The following seasonal categories were used for analysis: winter (December–February), spring (March–May), summer (June–August), and autumn (September–November).
Case definition.
The Sonora MOH defines a case of RMSF as abrupt onset of fever (> 38.5°C), plus at least two of the following clinical features: headache, rash, myalgia, malaise, meningismus, hemorrhage, purpura, hyponatremia, leukocytosis, leukopenia, thrombocytopenia, elevated hepatic transaminases, elevated lactate dehydrogenase, and shock. Cases must also satisfy one of the following epidemiologic criteria: 1) history of tick bite or contact with tick-infested dog in the 2 weeks preceding onset of symptoms, 2) ticks present in or around the house, or 3) travel to or residing in a neighborhood with an identified case of RMSF within the previous 6-month period. A confirmed case requires one of the following laboratory findings: 1) R. rickettsii DNA detected in a whole blood sample via PCR assay, or 2) single IgM or IgG antibody titer of ≥ 1:64 reactive to R. rickettsii antigen by indirect immunofluorescence antibody assay (IFA). A case is considered probable if the clinical criteria are satisfied, but no confirmatory laboratory evidence is available. All confirmed and probable cases were included in this analysis.
Statistical analysis.
Descriptive statistics, RRs, and corresponding 95% CIs and P-values were calculated for all variables to assess association with fatal outcome. Categorical data are presented as proportions and compared using Pearson’s chi-square test or Fisher’s exact test when any cell contained fewer than five observations, as appropriate. Normally distributed continuous variables are presented as means (SDs) and compared using Student’s t-test, whereas nonnormally distributed continuous variables are presented as medians (interquartile ranges [IQRs]) and compared using the Mann–Whitney/Wilcoxon two-sample test, as appropriate. Two-sided statistical tests were considered significant at α = 0.05. All data analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC).
Mapping.
Maps were created using ArcGIS Desktop 10.5.1 (ESRI, Redlands, CA). Pie charts were made proportionate to the number of cases represented, and fatal and nonfatal cases were represented for each jurisdiction. In addition, optimized hot spot analysis in Getis-Ord Gi* was used to identify hot spots of disease. This analysis identifies an appropriate geographic scale of analysis and clusters of disease by determining where a feature (e.g., municipalities) with a high value is surrounded by other features with lower values.
Ethics statement.
All data were previously collected for national surveillance purposes and was de-identified and aggregated. As such, a full ethical review was deemed unnecessary by both institutions.
RESULTS
Demographics and exposure.
During 2015–2018, a total of 510 cases of RMSF were reported; 432 (85%) were confirmed and 78 (15%) were probable (Table 1). Of all case patients, 263 (52%) were male and 23 (5%) self-identified as part of indigenous communities. The median age was 19 (IQR: 10–42) years. Case patients were further stratified by age-group with the highest number of reported cases occurring in children aged 8–18 years (n = 174; 34%) and adults aged 36–64 (n = 145; 28%) years.
Demographic and treatment characteristics of Rocky Mountain spotted fever case patients by fatal and nonfatal outcome, 2015–2018
| Overall cases | Fatal cases | Nonfatal cases | RR (95% CI) | P-value | |
|---|---|---|---|---|---|
| N = 510 (%) | n = 222 (%) | n = 288 (%) | |||
| Gender | |||||
| Male | 263 (52) | 128 (49) | 135 (51) | 1.28 (1.05–1.56) | 0.02 |
| Female | 247 (48) | 94 (38) | 153 (62) | Ref | – |
| Age-group (years) | |||||
| < 8 | 78 (15) | 21 (27) | 57 (73) | 0.82 (0.54–1.25) | 0.36 |
| 8–18 | 174 (34) | 57 (33) | 117 (67) | Ref | – |
| 19–35 | 101 (20) | 52 (51) | 49 (49) | 1.57 (1.18–2.09) | < 0.01 |
| 36–64 | 145 (28) | 84 (58) | 61 (42) | 1.77 (1.37–2.28) | < 0.01 |
| 65+ | 12 (2) | 8 (67) | 4 (33) | 2.04 (1.29–3.2) | 0.03 |
| Median (interquartile range) | 19 (10–42) | 30 (14–46) | 15 (8–31) | – | < 0.0001 |
| Ethnicity | |||||
| Indigenous | 23 (5) | 12 (52) | 11 (48) | 1.22 (0.81–1.83) | 0.38 |
| Nonindigenous | 481 (94) | 206 (43) | 275 (57) | Ref | – |
| Unknown | 6 (1) | 4 (67) | 2 (33) | 1.56 (0.88–2.77) | 0.41 |
| Jurisdiction | |||||
| Hermosillo | 214 (42) | 77 (36) | 137 (64) | Ref | – |
| Caborca | 19 (4) | 10 (53) | 9 (47) | 1.46 (0.92–2.32) | 0.15 |
| Santa Ana | 24 (5) | 13 (54) | 11 (46) | 1.51 (1.00–2.27) | 0.08 |
| Ciudad Obregon | 141 (28) | 73 (52) | 68 (48) | 1.44 (1.13–1.83) | < 0.01 |
| Navojoa | 107 (21) | 45 (42) | 62 (58) | 1.17 (0.88–1.55) | 0.29 |
| San Luis Rio Colorado | 5 (1) | 4 (80) | 1 (20) | 2.22 (1.39–3.57) | 0.06 |
| Season of onset | |||||
| December–February | 88 (17) | 50 (57) | 38 (43) | 1.42 (1.09–1.84) | 0.01 |
| March–May | 105 (21) | 43 (41) | 62 (59) | 1.02 (0.76–1.38) | 0.88 |
| June–August | 152 (30) | 63 (41) | 89 (59) | 1.04 (0.79–1.35) | 0.79 |
| September–November | 165 (32) | 66 (40) | 99 (60) | Ref | – |
| Exposures | |||||
| Tick exposure reported | 407 (80) | 183 (45) | 224 (55) | 1.32 (0.95–1.82) | 0.08 |
| Dog contact reported | 452 (89) | 190 (42) | 262 (58) | 0.75 (0.57–0.98) | 0.06 |
| Recent history of unexplained death of family dog | 29 (7) | 13 (45) | 16 (55) | 1.04 (0.69–1.59) | 0.84 |
| Fever, rash, and tick exposure | 305 (60) | 135 (44) | 170 (56) | 1.04 (0.85–1.28) | 0.68 |
| Case definition | |||||
| Confirmed | 432 (85) | 169 (39) | 263 (61) | 0.58 (0.47–0.70) | < 0.01 |
| Probable | 78 (15) | 53 (68) | 25 (32) | Ref | – |
| Diagnostic method | |||||
| PCR | 323 (63) | 90 (49) | 94 (51) | Ref | – |
| IFA | 109 (21) | 13 (12) | 96 (88) | 0.24 (0.14–0.41) | < 0.01 |
| Clinical symptoms | 78 (15) | 53 (68) | 25 (32) | 1.39 (1.12–1.72) | < 0.01 |
| Treatment | |||||
| Received doxycycline | 444 (87) | 197 (44) | 247 (56) | 1.15 (0.83–1.60) | 0.37 |
| Onset of symptoms to (mean days [SD])* | |||||
| Seeking care (n = 507) | 5.4 (4.5) | 5.5 (2.9) | 5.2 (5.4) | – | 0.43 |
| Treatment (n = 444) | 7.9 (5.5) | 7.4 (4.0) | 8.3 (6.4) | – | 0.09 |
| Death (n = 222) | – | 9.3 (24.6) | – | – | – |
| Sample collection (n = 473) | 6.5 (4.9) | 6.0 (2.9) | 6.9 (5.9) | – | 0.05 |
| PCR diagnosed | 5.3 (4.0) | 5.5 (2.4) | 5.1 (5.0) | – | 0.39 |
| IFA diagnosed | 9.3 (5.3) | 8.8 (4.9) | 9.3 (5.4) | – | 0.38 |
| Seeking care to treatment (n = 359)* | 4.2 (6.0) | 3.3 (4.3) | 4.9 (6.9) | – | < 0.0001 |
IFA = indirect immunofluorescence antibody assay; Ref = reference group.
“Time to” variables included observations where illness onset date was reported to precede a given outcome.
During the study period, the highest proportion of cases reported illness onset in 2015 (n = 180, 35%); 85 (48%) were fatal (Figure 1). Cases were distributed throughout all months of the year, with the highest proportion of cases reported in August (n = 56, 11%), September (n = 63, 12%), and October (n = 64, 13%) (Figure 2).

Reported cases of Rocky Mountain spotted fever and case fatality rates (CFRs) by year—Sonora, Mexico, 2015–2018.
Citation: The American Journal of Tropical Medicine and Hygiene 104, 1; 10.4269/ajtmh.20-0854
Cases of Rocky Mountain spotted fever by month of illness onset and corresponding case fatality rate by month—Sonora, Mexico, 2015–2018.
Citation: The American Journal of Tropical Medicine and Hygiene 104, 1; 10.4269/ajtmh.20-0854
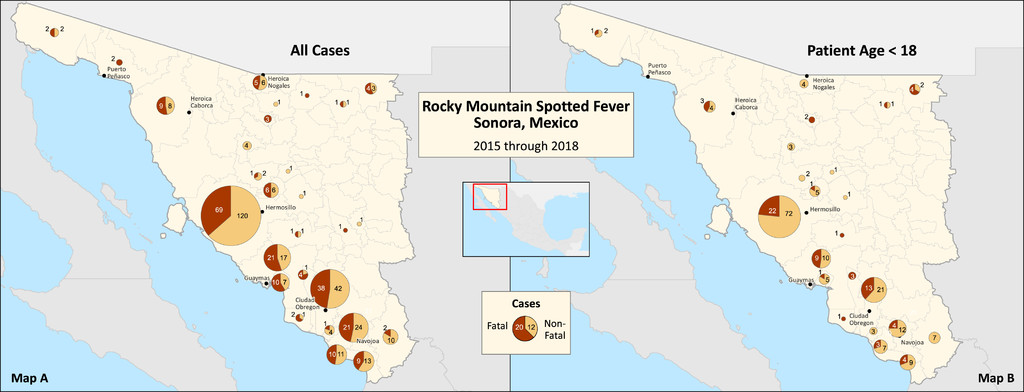
When characterized by geographical location, Hermosillo (Jurisdiction 1) reported the largest number of cases (n = 214, 42%), followed by Ciudad Obregon (Jurisdiction 4; n = 141, 28%) and Navojoa (Jurisdiction 5; n = 107, 21%) (Figure 3). Exposure to ticks (n = 407, 80%) and contact with dogs (n = 452, 89%) were reported in most cases. Few cases (n = 29, 7%) reported recent history of unusual dog death. More than half (60%) of cases reported the triad of fever, rash, and tick exposure (Table 1).
Proportion of fatal and nonfatal cases of Rocky Mountain spotted fever in Sonora, Mexico, 2015–2018, among all cases (Map A) and persons aged < 18 years (Map B).
Citation: The American Journal of Tropical Medicine and Hygiene 104, 1; 10.4269/ajtmh.20-0854
Clinical and laboratory findings.
Fever was reported by all cases as required by the case definition. The most common clinical symptoms were headache (93%), myalgia (90%), mild to moderate arthralgia (79%), rash (67%), and nausea (57%) (Table 2). Of the 67% of case patients with rash during the course of illness, pediatric cases (aged ≤ 18 years) reported rash with higher frequency than adults (80% versus 55%, RR = 1.43; CI: 1.26–1.62; P < 0.01) (Table 2).
Clinical findings: Cases of Rocky Mountain spotted fever—Sonora, Mexico 2015–2018
| Sign/symptom | Overall cases | Fatal cases | Nonfatal cases | RR (95% CI) | P-value | Pediatric cases | Adult cases | RR (95% CI) | P-value |
|---|---|---|---|---|---|---|---|---|---|
| N = 510 (100%) | n = 222 (44%) | n = 288 (56%) | n = 244 (48%) | n = 266 (52%) | |||||
| Fever | 510 (100) | 222 (100) | 288 (100) | – | – | 244 (100) | 266 (100) | – | – |
| Headache | 473 (93) | 205 (92) | 268 (93) | 0.94 (0.66–1.36) | 0.76 | 222 (91) | 251 (94) | 0.96 (0.92–1.01) | 0.14 |
| Myalgia | 460 (90) | 202 (91) | 258 (90) | 1.10 (0.77–1.57) | 0.60 | 215 (88) | 245 (92) | 0.96 (0.90–1.01) | 0.13 |
| Mild to moderate arthralgia | 402 (79) | 186 (84) | 216 (75) | 1.39 (1.04–1.85) | 0.02 | 186 (76) | 216 (81) | 0.94 (0.86–1.03) | 0.17 |
| Rash | 342 (67) | 144 (66) | 198 (69) | 0.93 (0.75–1.14) | 0.48 | 195 (80) | 147 (55) | 1.43 (1.26–1.62) | < 0.01 |
| Nausea | 288 (57) | 122 (55) | 166 (58) | 0.93 (0.77–1.14) | 0.50 | 138 (57) | 150 (56) | 1.00 (0.86–1.17) | 0.96 |
| Vomiting | 243 (48) | 113 (52) | 130 (46) | 1.14 (0.93–1.39) | 0.20 | 127 (52) | 116 (44) | 1.19 (0.99–1.43) | 0.06 |
| Chills | 222 (44) | 98 (45) | 124 (44) | 1.02 (0.84–1.25) | 0.84 | 89 (36) | 133 (50) | 0.73 (0.60–0.90) | < 0.01 |
| Diarrhea | 127 (25) | 68 (31) | 59 (21) | 1.33 (1.08–1.63) | 0.01 | 51 (21) | 76 (29) | 0.73 (0.54–1.00) | 0.05 |
| Edema | 77 (20) | 41 (24) | 36 (17) | 1.25 (1.00–1.60) | 0.09 | 42 (17) | 35 (13) | 1.39 (0.93–2.08) | 0.10 |
| Dyspnea | 82 (16) | 55 (25) | 27 (10) | 1.73 (1.42–2.10) | < 0.01 | 31 (13) | 51 (19) | 0.66 (0.44–0.99) | 0.04 |
| Disorientation | 81 (16) | 55 (26) | 26 (9) | 1.77 (1.46–2.14) | < 0.01 | 32 (13) | 49 (18) | 0.71 (0.47–1.07) | 0.10 |
| Stupor | 53 (10) | 36 (17) | 17 (6) | 1.68 (1.36–2.09) | < 0.01 | 21 (9) | 32 (12) | 0.71 (0.42–1.19) | 0.19 |
| Severe polyarthralgia | 50 (10) | 13 (6) | 37 (13) | 0.57 (0.35–0.92) | < 0.01 | 18 (7) | 32 (12) | 0.61 (0.35–1.06) | 0.08 |
| Lethargy | 47 (9) | 29 (14) | 18 (7) | 1.49 (1.16–1.91) | < 0.01 | 25 (10) | 22 (8) | 1.27 (0.74–2.20) | 0.38 |
| Shock | 44 (9) | 28 (13) | 16 (6) | 1.54 (1.20–1.98) | < 0.01 | 27 (11) | 17 (6) | 1.77 (0.99–3.17) | 0.05 |
| Hemorrhage | 43 (8) | 31 (16) | 12 (5) | 1.74 (1.39–2.17) | < 0.01 | 18 (7) | 25 (9) | 0.73 (0.41–1.30) | 0.29 |
| Tremors | 39 (8) | 21 (10) | 18 (6) | 1.28 (0.94–1.74) | 0.16 | 14 (6) | 25 (9) | 0.61 (0.32–1.14) | 0.12 |
| Jaundice | 35 (7) | 22 (10) | 13 (5) | 1.50 (1.14–1.98) | 0.02 | 10 (4) | 25 (9) | 0.43 (0.21–0.88) | 0.02 |
| Arthritis | 32 (6) | 6 (3) | 26 (9) | 0.42 (0.20–0.87) | < 0.01 | 13 (5) | 19 (7) | 0.74 (0.37–1.46) | 0.38 |
| Seizures | 27 (5) | 23 (11) | 4 (1) | 2.09 (1.73–2.53) | < 0.01 | 15 (6) | 12 (5) | 1.35 (0.65–2.83) | 0.42 |
Median platelet count was below the lower limit of normal (30,000 × 103 platelets/µL, IQR: 14,850–71,000). Median creatinine (1.8 mEq/L, IQR: 0.8–3.2) and total bilirubin (2.9 mg/dL, IQR: 1.5–5.0) levels were above the upper limits of normal. Median aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels were elevated in reported cases (AST: 198.1 IU/L, IQR: 117.0–348.1; ALT: 87.5 IU/L, IQR: 54.0–125.0) (Table 3).
Laboratory diagnostics in fatal and nonfatal cases of Rocky Mountain spotted fever—Sonora, Mexico 2015–2018
| Median laboratory values (interquartile range) | |||||
|---|---|---|---|---|---|
| Laboratory test | Fatal cases | n | Nonfatal cases | N | P-value |
| White blood cell count (×103 cells/mL) | 10.8 (7.2–16.7) | 197 | 8.5 (6.2–12.3) | 144 | < 0.01 |
| Neutrophils (%) | 89.5 (82.0–92.5) | 140 | 82.0 (70.0–87.0) | 58 | < 0.0001 |
| Hemoglobin (g/dL) | 13.4 (12.2–14.5) | 197 | 12.3 (10.9–13.3) | 180 | < 0.0001 |
| Hematocrit (%) | 39.0 (35.2–43.1) | 193 | 35.7 (31.6–38.6) | 178 | < 0.0001 |
| Platelet count (×103 platelets/mL) | 18,000 (11,000–34,900) | 209 | 52,000 (23,000–110,000) | 207 | < 0.0001 |
| Sodium (mEq/L) | 131.0 (124.0–136.0) | 83 | 132.0 (128.0–135.0) | 57 | 0.54 |
| Creatinine (mEq/L) | 2.3 (1.2–3.4) | 132 | 0.7 (0.4–1.4) | 48 | < 0.0001 |
| Serum glutamic oxaloacetic transaminase/aspartate aminotransferase (IU/L) | 256 (151–408) | 147 | 134 (80–215) | 87 | < 0.0001 |
| Serum glutamic pyruvic transaminase/alanine aminotransferase (IU/L) | 95.5 (69.0–146.0) | 146 | 69.5 (47.0–92.0) | 84 | < 0.0001 |
| Total bilirubin (mg/dL) | 3.7 (2.4–5.7) | 147 | 1.6 (0.8–2.6) | 72 | < 0.0001 |
Sixty-three percent (n = 323) of all cases were diagnosed by PCR, 21% (n = 109) were diagnosed by IFA, and 78 (15%) did not have laboratory results. Of those patients diagnosed by PCR, the mean time from illness onset to specimen collection was 5.3 days (SD = 4.0); of those patients diagnosed by IFA, the mean time was 9.3 days (SD = 5.3) (Table 1).
Case fatality.
A total of 222 case patients died during the study period, for a CFR of 44%. The median age among fatal cases was 30 (IQR: 14–46) years. All age-groups experienced CFRs greater than 25%; the age-group with the highest fatality rate was case patients aged 65 years or older (67%), followed by 36–64 years (58%). The CFR was lowest (27%) for those aged < 8 years. Case fatality rate was higher among males than females (49% versus 38%, RR = 1.28; CI: 1.05–1.56; P = 0.02). Confirmed cases were less likely than probable cases to result in fatal outcome (RR = 0.58; CI: 0.47–0.70; P < 0.01) (Table 1).
The reported CFR was highest in 2015 (47%) (Figure 1). Those with illness onset during December–February were significantly more likely to have fatal outcome than cases with illness onset during September–November (57% versus 40%, RR = 1.42; CI: 1.09–1.84; P = 0.01) (Table 1). The highest CFR was reported in the month of March (13%) (Figure 2).
The jurisdiction with the highest number of fatal cases was Hermosillo (Jurisdiction 1; n = 77); however, it had the lowest CFR (36%) because it is also the most populous jurisdiction. When comparing jurisdictions, Ciudad Obregon (Jurisdiction 4) had a significantly higher risk of a case having a fatal outcome (RR = 1.44; CI: 1.13–1.83; P < 0.01) than Hermosillo (Jurisdiction 1). Risk factors, such as exposure to ticks (RR = 1.32; CI: 0.95–1.82; P = 0.08), contact with dogs (RR = 0.75; CI: 0.57–1.59; P = 0.06), and recent history of an unusual dog death (RR = 1.04; CI: 0.69–1.59; P = 0.84), did not differ significantly between fatal and nonfatal cases (Table 1). The presence of the triad of fever, exposure to tick, and rash was not significantly different between fatal and nonfatal cases (44% versus 56%, RR = 1.04; CI: 0.85–1.28; P = 0.68).
The mean (M) time from symptom onset to seeking care was 5.4 days (SD ± 4.5); there was not a significant difference between fatal (M = 5.5; SD = 2.9) and nonfatal cases (M = 5.2; SD = 5.4; P = 0.43) (Table 4). The symptoms significantly associated with fatal outcome were mild to moderate arthralgia (RR = 1.39; CI: 1.04–1.85; P = 0.02), dyspnea (RR = 1.73; CI: 1.42–2.10; P < 0.01), disorientation (RR = 1.77; CI: 1.46–2.14; P < 0.01), stupor (RR = 1.68; CI: 1.36–2.09; P < 0.01), lethargy (RR = 1.49; CI: 1.16–1.91; P < 0.01), shock (RR = 1.54; CI: 1.20–1.98; P < 0.01), hemorrhage (RR = 1.74; CI 1.39–2.17; P < 0.01), jaundice (RR = 1.50; CI: 1.14–1.98; P = 0.02), and seizures (RR = 2.09; CI: 1.73–2.53; P < 0.01) (Table 2). The mean time from onset of symptoms to death was 9.3 days (SD ± 24.6).
Treatment of Rocky Mountain spotted fever—Sonora, Mexico 2015–2018
| Overall treated | Doxy treatment ≤ 5 days | Doxy treatment > 5 days | RR (95% CI) | P-value | |
|---|---|---|---|---|---|
| N = 444 (87%) | n = 142 (32%) | n = 302 (68%) | |||
| Age-group (years) | |||||
| < 8 | 69 (16) | 26 (38) | 43 (62) | 1.23 (0.83–1.80) | 0.31 |
| 8–18 | 153 (34) | 47 (31) | 106 (69) | Ref | – |
| 19–35 | 83 (19) | 22 (27) | 61 (73) | 0.86 (0.56–1.33) | 0.50 |
| 36–64 | 129 (29) | 43 (33) | 86 (67) | 1.09 (0.77–1.53) | 0.64 |
| > 65 | 10 (2) | 4 (40) | 6 (60) | 1.30 (0.59–2.89) | 0.51 |
| Gender | |||||
| Male | 227 (51) | 70 (31) | 157 (69) | 0.93 (0.71–1.22) | 0.60 |
| Female | 217 (49) | 72 (33) | 145 (67) | Ref | – |
| Jurisdiction | |||||
| Hermosillo | 185 (42) | 63 (34) | 122 (66) | Ref | – |
| Caborca | 15 (3) | 4 (27) | 11 (73) | 0.78 (0.33–1.86) | 0.56 |
| Santa Ana | 21 (5) | 8 (38) | 13 (62) | 1.12 (0.63–2.0) | 0.71 |
| Ciudad Obregon | 127 (29) | 34 (27) | 93 (73) | 0.79 (0.55–1.12) | 0.17 |
| Navojoa | 92 (21) | 32 (35) | 60 (65) | 1.02 (0.72–1.44) | 0.90 |
| San Luis Rio Colorado | 4 (1) | 1 (25) | 3 (75) | 0.73 (0.13–4.06) | 0.71 |
| Season of onset | |||||
| December–February | 72 (16) | 18 (25) | 54 (75) | 0.71 (0.45–1.11) | 0.12 |
| March–May | 92 (21) | 22 (24) | 70 (76) | 0.68 (0.44–1.03) | 0.06 |
| June–August | 133 (30) | 50 (38) | 83 (62) | 1.06 (0.78–1.45) | 0.70 |
| September–November | 147 (33) | 52 (25) | 95 (65) | Ref | – |
| Ethnicity | |||||
| Indigenous | 21 (5) | 8 (38) | 13 (62) | 1.22 (0.69–2.14) | 0.63 |
| Nonindigenous | 418 (94) | 131 (31) | 287 (69) | Ref | – |
| Unknown | 5 (1) | 3 (60) | 2 (40) | 1.91 (0.92–3.97) | 0.33 |
| Case definition | |||||
| Confirmed | 379 (85) | 124 (33) | 255 (67) | 1.18 (0.78–1.80) | 0.42 |
| Probable | 65 (15) | 18 (28) | 47 (72) | Ref | – |
| Diagnostic method | |||||
| PCR | 287 (65) | 109 (38) | 178 (62) | Ref | – |
| Immunofluorescence antibody assay | 92 (21) | 15 (16) | 77 (84) | 0.43 (0.26–0.70) | < 0.01 |
| Clinical symptoms | 65 (15) | 18 (28) | 47 (71) | 0.73 (0.48–1.11) | 0.12 |
Ref = reference group.
Median platelet counts were significantly lower among fatal cases (18,000 × 103 platelets/µL, IQR: 11,000–34,900) than nonfatal cases (52,000 × 103 platelets/µL, IQR: 23,000–110,000; P < 0.0001) (Table 3). Median creatinine levels were significantly higher in fatal cases (2.3 mEq/L, IQR: 1.2–3.4) than nonfatal cases (0.7 mEq/L, IQR: 0.4–1.4; P < 0.0001) (Table 3).
Case patients diagnosed by IFA were significantly less likely to have fatal outcome than case patients diagnosed by PCR (RR = 0.24; CI: 0.14–0.41; P < 0.01). Those diagnosed by clinical symptoms alone were significantly more likely to have fatal outcome than those diagnosed by PCR (RR = 1.39; CI: 1.12–1.72; P < 0.01).
Treatment.
Most patients (n = 444, 87%) were treated with doxycycline. The mean time from onset of symptoms to treatment was 7.9 days (SD ± 5.5). Of those receiving doxycycline, only 32% (n = 142) received it within the first 5 days of illness. Within each age-group, fewer than half of case patients received doxycycline within 5 days of illness onset; only 38% of those aged < 8 years received doxycycline within 5 days of illness onset (Table 4). There were no significant differences seen between jurisdiction of residence and receipt of doxycycline within the recommended time frame. The season of onset was found to have a significant association, and developing symptoms during March–May increased chances of being treated within 5 days of illness onset (RR = 0.68; P-value 0.06). A smaller proportion of cases diagnosed by IFA received doxycycline within 5 days than those diagnosed by PCR (P < 0.01) (Table 4).
Time from onset of symptoms to treatment was beyond the recommended 5-day window for both fatal and nonfatal cases, whereas time to treatment was less for fatal cases (M = 7.4; SD ± 4.0) than for nonfatal cases (M = 8.3; SD ± 6.4); the difference was not statistically significant (RR = 1.15; CI: 0.83–1.60; P = 0.37) (Table 1).
Mapping and hot spot analysis.
Mapping of cases by municipality revealed two areas of case concentration, which are also population hubs: one near Hermosillo, and the other in the southwestern region of the state. Case fatality rate varied across all cases and in those aged ≤ 18 years, with the lowest CFR in Hermosillo and highest in the southern portion of the state. The maps comparing CFR by region in adults and those aged ≤ 18 years showed a lower CFR in those aged ≤ 18 years across all regions (Figure 3). When adjusting for population by municipality, the hot spot analysis revealed neither areas of inordinately high nor low incidence, with increased incidence of disease concentrating in regions of high population.
DISCUSSION
Rocky Mountain spotted fever remains a prominent threat in Sonora, with 510 cases reported in four years. A significant portion (49%) of these cases is still being reported in children aged ≤ 18 years. Even more concerning is the alarmingly high CFR of 44%, even when with the pre-antibiotic era in the United States. 20,22 At the beginning of the RMSF epidemic in Sonora, children aged < 8 years had the highest CFR. However, current data show this has declined, and in our study, this age-group had the lowest CFR among all age-groups. The decrease in CFR among children may be attributed to interventions by local health authorities in Sonora such as 1) availability of intravenous doxycycline in hospitals, 2) clinical education targeting early recognition and treatment, 3) enhanced epidemiological surveillance to understand gaps in practice and detect trends earlier, 4) vector control programs, and 5) community health promotion programs focused on responsible pet ownership and reduction of tick burden on dogs. 23 By contrast, the high CFR among individuals aged ≥ 65 years may be attributable to comorbid conditions and less concerted effort by providers to consider RMSF in the differential for an adult patient presenting with febrile illness. It is also possible that these individuals are less familiar with RMSF, given its only recent emergence in the community, and thus less likely to perceive ticks as high risk. 24
Despite previous studies showing little predictive utility in laboratory values among adults, we found certain results to be helpful and of clinical utility in predicting fatal outcome. 25,26 A study conducted in an Arizona tribal community found that laboratory results did not differ between confirmed RMSF cases and non-confirmed cases. 26 Another study among the same population found only elevated liver function tests to be helpful in predicting fatal outcome. 27 In this study, we add that the presence of severe thrombocytopenia and elevated creatinine are associated with fatal outcome. The median laboratory values differed substantially enough that a provider could consider a platelet value of < 23,000 × 103 platelets/µL or a creatinine level > 1.4 to be highly predictive of fatal outcome.
Time from symptom onset to seeking care was longer than that in previous studies and represents an opportunity for increased community education and awareness. 26 Treatment is most effective within the first 5 days of illness; because most patients sought care on or after day 5 of illness, even prompt recognition and treatment by healthcare providers may not be effective at reducing mortality. However, treatment was also frequently delayed 3–4 days after initial healthcare contact. This undoubtedly contributes to the high mortality seen among RMSF case patients in Sonora and demonstrates a need for continued education among providers, especially in endemic areas of key importance.
Geographic location was notable in both prevalence and CFR. Cases are most numerous in urban centers likely because of the larger population at risk. Interestingly, the hot spot analysis revealed that when adjusting for population size at the level of the municipality, there were neither areas of particularly high nor low incidence. Geography became more significant in relation to CFR, with the lowest appreciated in Jurisdiction 1 and the highest in Jurisdictions 4 and 5 located in the southern portion of the state. It is also notable that despite similar sociodemographic conditions, climate, and comparable populations of free-roaming dogs, the CFR in Sonora is six times higher than that in tribal regions in the United States. 26 Factors that may contribute to disproportionately high CFRs both in Sonora and within the state are delay in clinical diagnosis and access to care. Such findings are consistent with previous studies conducted in different regions. 2,25 When comparing with Sonora’s other health jurisdictions, Hermosillo’s lower CFR may be due to overall better socioeconomic conditions, improved provider education and awareness, and access to health care. By contrast, the south of Sonora experiences higher rates of social deprivation and a more rural distribution of the population. 28 These can all contribute to difficulty accessing medical care, poor provider awareness, and delayed treatment. 20
PCR-confirmed cases were more likely to experience a fatal outcome than cases confirmed by serology. Although elevated serologic titers can reflect past exposure, PCR confirmation is more indicative of the etiology of the current infection. Our results confirm those with PCR confirmation had a higher CFR; however, the CFR of 49% seen in this cohort exceeds the pre-doxycycline era. This suggests that additional factors are contributing to an inordinately high CFR; these can include pathogen (e.g., virulent strain), vector (e.g., brown dog tick), host (e.g., malnutrition), or biased sampling (e.g., surveillance capture of severe cases). Treatment should be initiated based on clinical suspicion and should not be delayed awaiting diagnostic confirmation. Because specimens for cases confirmed by PCR were collected at a mean of 5.3 days, this highlights the importance of education providers to begin treatment when suspecting RMSF and not to await confirmatory diagnostic results.
Seasonality was also significant in our analysis. Cases were evenly distributed throughout the year, but CFR was highest during March. Because we also observed the highest proportion of untreated cases in winter, we suspect other etiologies were being considered more highly, such as influenza or respiratory syncytial virus infection. Providers may also have misconceptions about the seasonality of RMSF, attributing highest risk to spring and summer months. 29 However, warmer temperatures (≥ 43°F), such as those in Sonora, increase winter activity of ticks, maintaining a high rate of exposure even during the winter months. 30 Providers in these areas should consider RMSF in their differential diagnosis even in the winter months.
This study is subject to a few limitations. PCR may be performed with more frequency on more severe cases as they may present for higher levels of care where molecular testing is more readily available. The current case definition allows a single titer of 1:64 to be sufficient evidence to confirm a case. This may represent previous exposure to any one of the spotted fever group Rickettsiae and may not be indicative of RMSF, placing more significance on the findings seen for PCR-confirmed cases. Furthermore, although this represents a more active approach to surveillance than standard laboratory-based pass surveillance, it is still likely we detected more severe cases, and this may underrepresent burden and overrepresent the most severe disease. Conversely, the probable case definition which relies on symptoms alone may be overly broad and not specific. Only 15% of cases were included on the basis of clinical criteria alone, so we feel this represents a small portion of the data. Last, missing data may bias the results and interpretation of trends.
The data captured through enhanced surveillance in Sonora provide reassuring evidence that education and targeted campaigns are effective in reversing disparities in CFR in pediatric populations. Treatment data also show more children are receiving the recommended doxycycline and that heightened awareness in adult populations is needed. It is concerning to see higher CFRs in areas of poverty and poorer access to care, and these should be targeted through additional training and education efforts. Our data also demonstrate a very significant finding that all populations are at equal risk for acquiring the disease, yet multiple modifiable factors can predict disposition.
ACKNOWLEDGMENTS
We would like to thank Elaine Hallisey from the Geospatial Research, Analysis, and Services Program at the Centers for Disease Control and Prevention for her assistance mapping and analyzing the geographic data.
REFERENCES
- 1.↑
Biggs HM et al. 2016. Diagnosis and management of tickborne rickettsial diseases: Rocky Mountain spotted fever and other spotted fever group rickettsioses, ehrlichioses, and anaplasmosis — United States. MMWR Recomm Rep 65: 1–44.
- 2.↑
Demma LJ et al. 2005. Rocky Mountain spotted fever from an unexpected tick vector in Arizona. N Engl J Med 353: 587–594.
- 3.
McQuiston JH , Guerra MA , Watts MR , Lawaczeck E , Levy C , Nicholson WL , Adjemian J , Swerdlow DL , 2011. Evidence of exposure to spotted fever group rickettsiae among Arizona dogs outside a previously documented outbreak area. Zoonoses Public Health 58: 85–92.
- 4.↑
Bustamante ME , Varela G , 1944. Characteristics of Rocky Mountain spotted fever in Sonora and Sinaloa, Mexico (study of 12 cases and 2 strains). Rev Inst Salub Enferm Trop 5: 129–134.
- 5.↑
Wikswo ME , Hu R , Metzger ME , Eremeeva ME , 2007. Detection of Rickettsia rickettsii and Bartonella henselae in Rhipicephalus sanguineus ticks from California. J Med Entomol 44: 158–162.
- 6.
Dantas-Torres F , 2008. The brown dog tick, Rhipicephalus sanguineus (Latreille, 1806) (Acari: Ixodidae): from taxonomy to control. Vet Parasitol 152: 173–185.
- 7.↑
Yaglom HD , Nicholson WL , Casal M , Nieto NC , Adams L , 2018. Serologic assessment for exposure to spotted fever group rickettsiae in dogs in the Arizona-Sonora border region. Zoonoses Public Health 65: 984–992.
- 8.↑
Dumler JS , Walker DH , 2005. Rocky Mountain spotted fever—changing ecology and persisting virulence. N Engl J Med 353: 551–533.
- 9.↑
Chen LF , Sexton DJ , 2008. What’s new in Rocky Mountain spotted fever? Infect Dis Clin North Am 22: 415–432, vii-viii.
- 10.↑
Gottlieb M , Long B , Koyfman A , 2018. The evaluation and management of Rocky Mountain spotted fever in the emergency department: a review of the literature. J Emerg Med 55: 42–50.
- 11.↑
Paddock CD , Alvarez-Hernández G , 2018. 178 – Rickettsia rickettsii (Rocky Mountain spotted fever). Long SS , Prober CG , Fischer M , eds. Principles and Practice of Pediatric Infectious Diseases, 5th edition. Philadelphia, PA: Elsevier, 952–957.e2.
- 13.
Buckingham SC , Marshall GS , Schutze GE , Woods CR , Jackson MA , Patterson LE , Jacobs RF ; Tick-borne Infections in Children Study Group , 2007. Clinical and laboratory features, hospital course, and outcome of Rocky Mountain spotted fever in children. J Pediatr 150: 180–184, 184 e1.
- 14.
Kirkland KB , Wilkinson WE , Sexton DJ , 1995. Therapeutic delay and mortality in cases of Rocky Mountain spotted fever. Clin Infect Dis 20: 1118–1121.
- 15.↑
CDC , 2000. Consequences of delayed diagnosis of Rocky Mountain spotted fever in children—West Virginia, Michigan, Tennessee, and Oklahoma, May–July 2000. MMWR Morb Mortal Wkly Rep 49: 885–888.
- 16.↑
Minniear TD , Buckingham SC , 2009. Managing Rocky Mountain spotted fever. Expert Rev Anti Infect Ther 7: 1131–1137.
- 17.↑
Todd SR , Dahlgren FS , Traeger MS , Beltran-Aguilar ED , Marianos DW , Hamilton C , McQuiston JH , Regan JJ , 2015. No visible dental staining in children treated with doxycycline for suspected Rocky Mountain spotted fever. J Pediatr 166: 1246–1251.
- 18.↑
Martinez-Medina MA , Padilla-Zamudio G , Solis-Gallardo LP , Guevara-Tovar M , 2005. Rocky Mountain spotted fever: report of two cases. Gac Med Mex 141: 309–312.
- 19.↑
Martinez-Medina MA , Alvarez-Hernandez G , Padilla-Zamudioa JG , Rojas-Guerra MG , 2007. Rocky Mountain spotted fever in children: clinical and epidemiological features. Gac Med Mex 143: 137–140.
- 20.↑
Álvarez-Hernández G , Roldán JFG , Milan NSH , Lash RR , Behravesh CB , Paddock CD , 2017. Rocky Mountain spotted fever in Mexico: past, present, and future. Lancet Infect Dis 17: e189–e196.
- 21.↑
Declaratoria de Emergencia Epidemiológica EE-1-2018. Subsecretaría de Prevención y Promoción de la Salud. CENAPRECE; México, D.F. 15 February 2018. Available at: http://www.cenaprece.salud.gob.mx/programas/interior/emergencias/descargas/pdf/1420.pdf.
- 22.↑
Delgado-De la Mora J , Licona-Enriquez JD , Leyva-Gastelum M , Delgado-De la Mora D , Rascon-Alcantar A , Alvarez-Hernandez G , 2018. A fatal case series of Rocky Mountain spotted fever in Sonora, Mexico. Biomedica 38: 69–76.
- 23.↑
Straily A , Drexler N , Cruz-Loustaunau D , Paddock CD , Alvarez-Hernandez G , 2016. Notes from the field: community-based prevention of Rocky Mountain spotted fever — Sonora, Mexico, 2016. MMWR Morb Mortal Wkly Rep 65: 1302–1303.
- 24.↑
Suárez R , Beltrán EM , Sánchez T , 2006. El sentido del riesgo desde la antropología médica: consonancias y disonancias con la salud pública en dos enfermedades transmisibles. Antípoda Revista de Antropología y Arqueología 3: 123–154. Available at: https://doi.org/10.7440/antipoda3.2006.05.
- 25.↑
Alvarez-Hernandez G , Murillo-Benitez C , Candia-Plata Mdel C , Moro M , 2015. Clinical profile and predictors of fatal Rocky Mountain spotted fever in children from Sonora, Mexico. Pediatr Infect Dis J 34: 125–130.
- 26.↑
Traeger MS et al. 2015. Rocky Mountain spotted fever characterization and comparison to similar illnesses in a highly endemic area—Arizona, 2002–2011. Clin Infect Dis 60: 1650–1658.
- 27.↑
Regan JJ et al. 2015. Risk factors for fatal outcome from Rocky Mountain spotted fever in a highly endemic area — Arizona, 2002–2011. Clin Infect Dis 60: 1659–1666.
- 28.↑
Garcia-Ochoa JJ , Ochoa-Vazquez I , Gonzalez-Velasquez L , Mendoza-Leon JG , 2015. Ranking of poverty in the municipalities of the state of Sonora, measured through the CONEVAL model, 2010. Rev Acad Sin Front 8: 21.
- 29.↑
Masters EJ , Olson GS , Weiner SJ , Paddock CD , 2003. Rocky Mountain spotted fever: a clinician’s dilemma. Arch Intern Med 163: 769–774.
- 30.↑
Suss J , Klaus C , Gerstengarbe FW , Werner PC , 2008. What makes ticks tick? Climate change, ticks, and tick-borne diseases. J Travel Med 15: 39–45.